
Report 79: mRNA COVID Vaccine-Induced Myocarditis at One Year Post-Injection: Spike Protein, Inflammation Still Present in Heart Tissue.
August 7, 2023 • by Robert W. Chandler, MD, MBA
In spite of widespread censorship, the truth is coming out that myocarditis arising after injection with mRNA COVID “vaccines” is notrare, temporary, or mild.
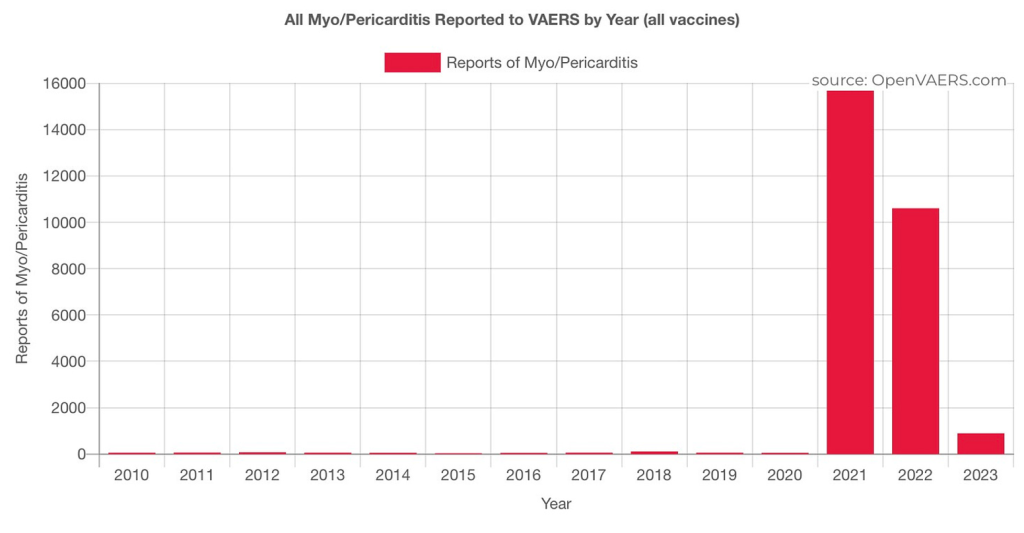
https://openvaers.com/covid-data/myo-pericarditis
Statement 1: Myocarditis after COVID-19 “vaccine” injection is rare.
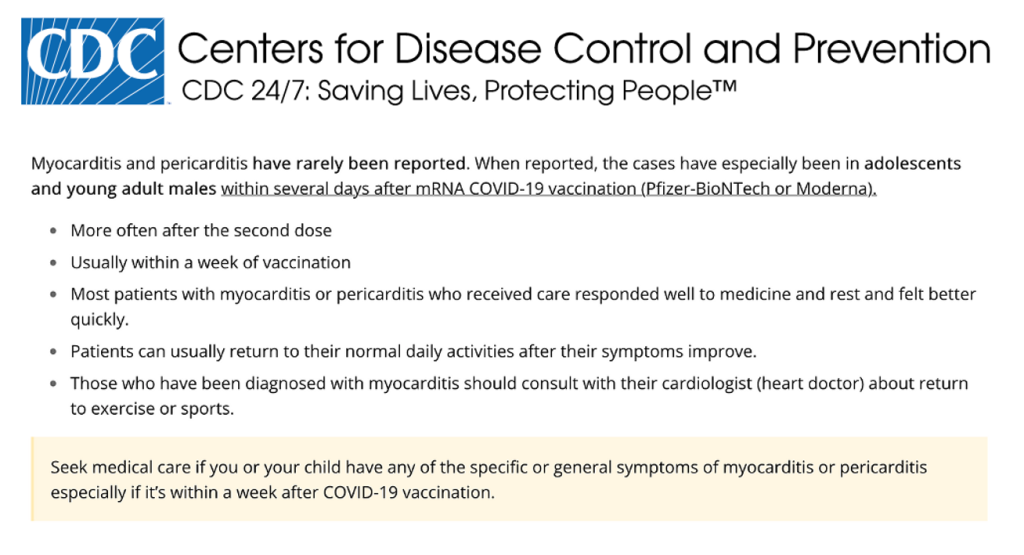
https://www.cdc.gov/coronavirus/2019-ncov/vaccines/safety/myocarditis.html
The Centers for Disease Control and Prevention’s (CDC) notice and its advice, above, ignore the following:
- Myocarditis post-mRNA COVID vaccine is not rare: 2.8% of 777 subjects studied prospectively were diagnosed with myocarditis, with a median age of 37, which is outside of the high-risk years. (Buergin et al., https://doi.org/10.1002/ejhf.2978.)
- According to the CDC’s Vaccine Adverse Events Reporting Systems (VAERS), 30% of myocarditis reports occur one week post-mRNA COVID injection. There is no basis upon which to make assumptions about when heart disease will appear with a drug that has biologic activity, like the mRNA COVID vaccines, and has never been used before. Proper studies were not done nor are they in progress at any scale.
- Return to normal activities after mRNA COVID vaccination and before cardiac diagnostic testing? NO! Just don’t do it.
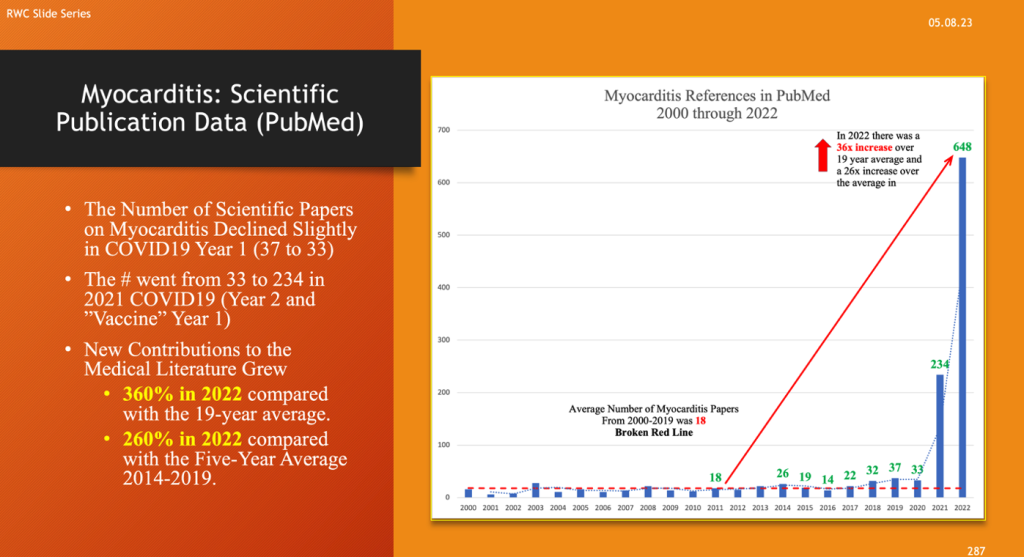
- The publication volume of medical literature concerning myocarditis declined slightly in 2020, the first year of COVID-19, from 37 reports in 2019 to 33 in 2020.
- In COVID “vaccine” Year 1/COVID-19 Year 2 (2021), the number of citations increased 13x compared with the 19-year average and 9x from the five-trailing-year average.
- In “vaccine” Year 2/COVID-19 Year 3 (2022), the number of citations increased 2.77x over the prior year, signaling a major medical event that continued after COVID died down and the injections slowed to a trickle.
- The cause can be sorted out in most myocarditis cases, and there is no reason to lump all myocarditis cases into the category of so-called “Long COVID.” Unless, of course, you want to hide the real cause.
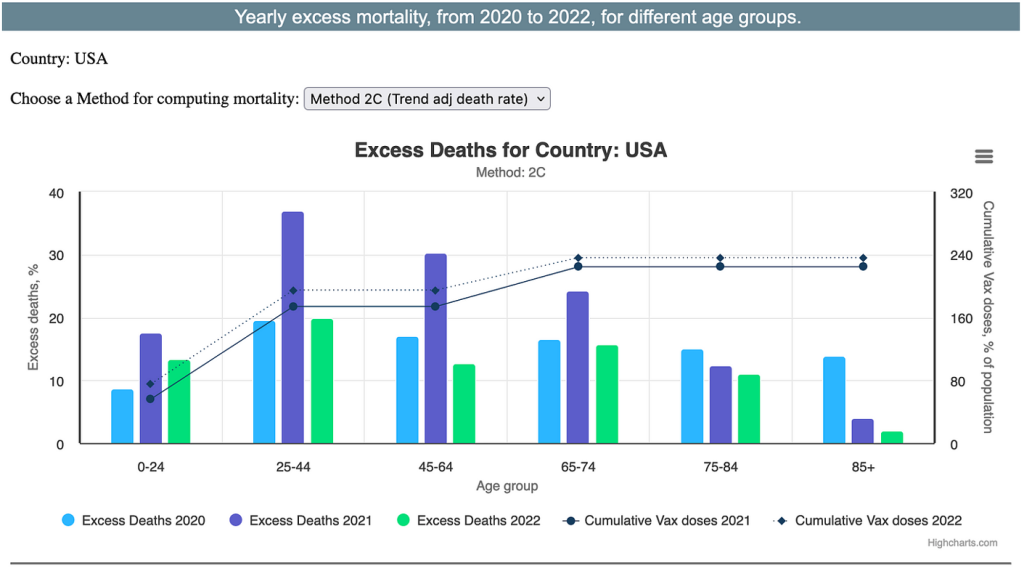
It is no surprise then to see the medical literature expand as excess deaths rise in both COVID and “vaccine” years, as indicated in Ed Dowd’s graph above. https://phinancetechnologies.com/HumanityProjects/Humanity%20Projects.asp
These are crude indicators when it comes to sorting out etiology of the excess deaths, and more comprehensive analyses are needed from the perspective of population studies down to aggregation of individual patient data.
Statement 2: Myocarditis after Spike-generating drug injection is temporary.
This statement has no scientific support. The Barmada et al. study found myo/pericardial damage in 14 out of 17 young people averaging 16.9 years of age. Young men comprising 87% of the group. At two months or longer follow-up, some patients had signs of worsening on their follow-up cMRI studies. (DOI: 10.1126/sciimmunol.adh3455)
Long-term, widespread study is required to estimate the magnitude of the problem of myo/pericarditis on a population level. Screening protocols with now identifiable sensitive and specific diagnostic techniques need to be deployed in a scalable program with built-in directed treatment.
Sudden death cases and unexpected fatalities require specific autopsies following the guidelines prepared by Dr. Arne Burkhardt.
https://dailyclout.io/wp-content/uploads/Burkhardt_Recipe_Updated.pdf
Few proper autopsies have been done. The slide below illustrates some of the findings of histopathological examination of the heart after mRNA COVID injection. Normal heart muscle is featured on the left and is juxtaposed with LNP/mRNA-damaged heart muscle on the right. The muscle structure is severely disrupted. There is infiltration of lymphocytes. The heart’s muscle cells are dead.
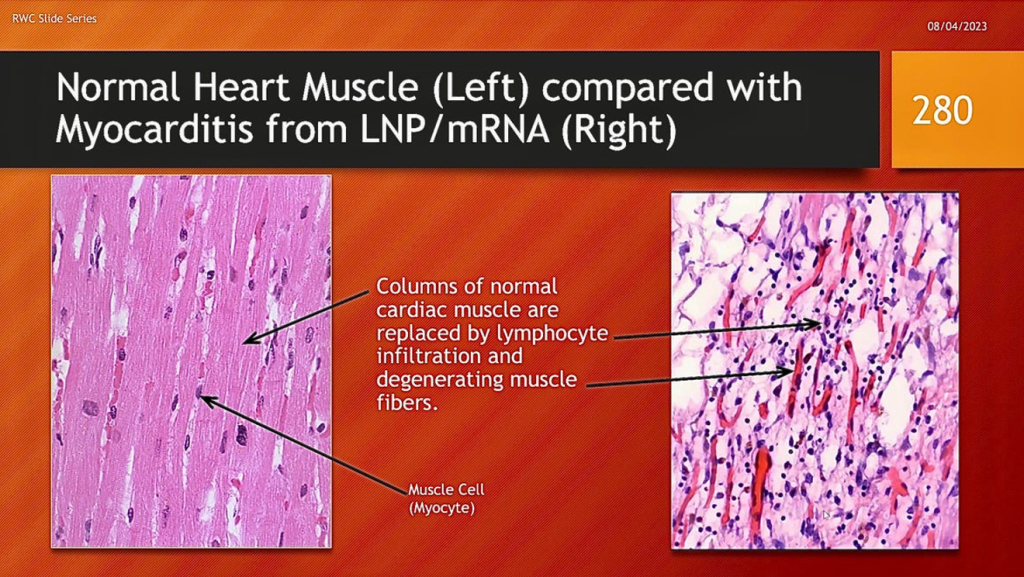
The exact process by which this destruction occurs has not been worked out at this point in time. Possibilities include an autoimmune reaction to modified host proteins, novel “vaccine”-induced non-self-proteins, molecular mimicry, or intense inflammatory reaction from mass cytokine release or complement cascade. Inflammation is a process that initiates healing, but it is also a process that can go out of control and destroy cells, tissues, and organs.
Early diagnosis and treatment are imperative. Acute phase diagnostics with inflammatory markers or signs of myocardial tissue damage, such as troponin, are necessary to make an accurate diagnosis. The graphic below is from Barmada et al. and shows how these indicators elevate with myocarditis.
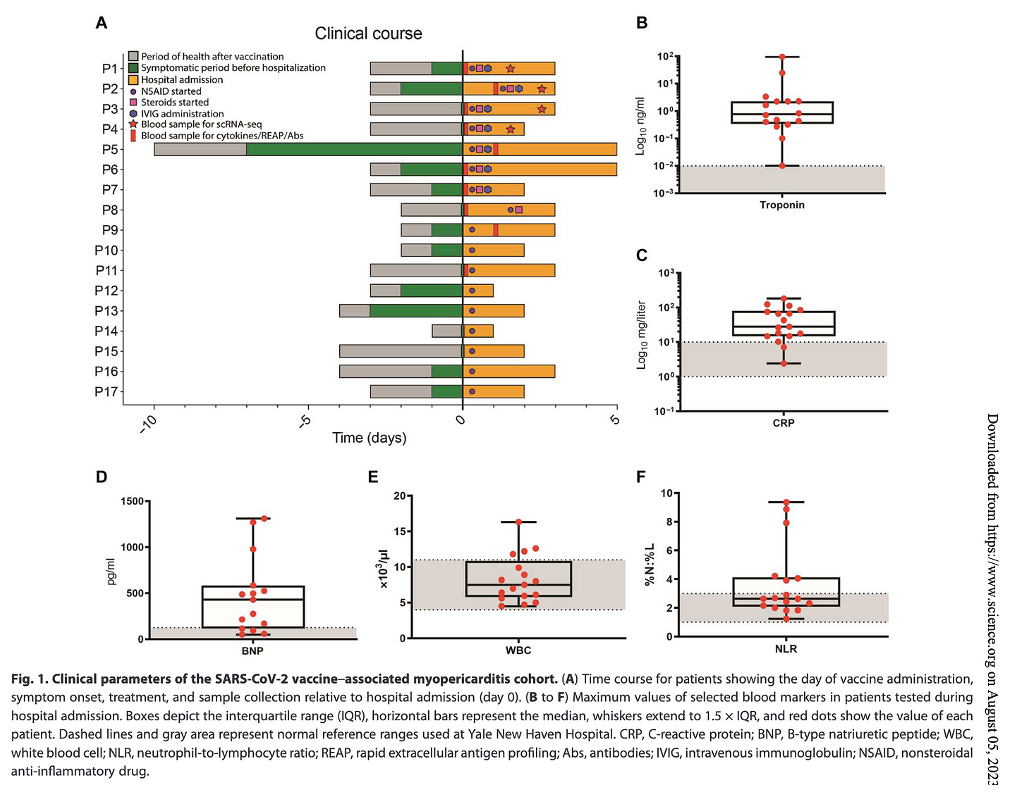
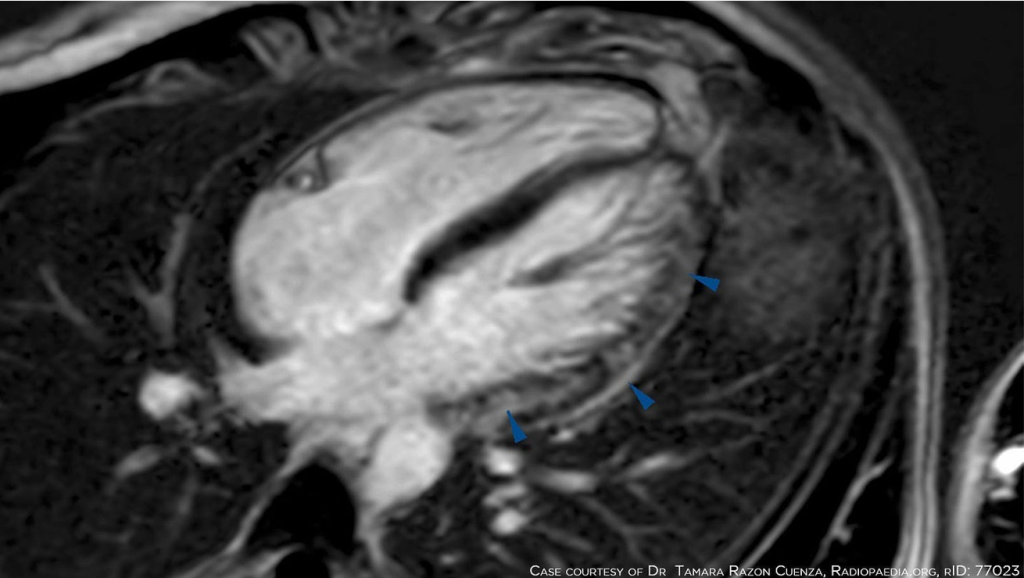
Cardiac MRI (cMRI) shows inflammatory change early and scarring once the inflammation subsides.
Statement Three: Myocarditis is mild.
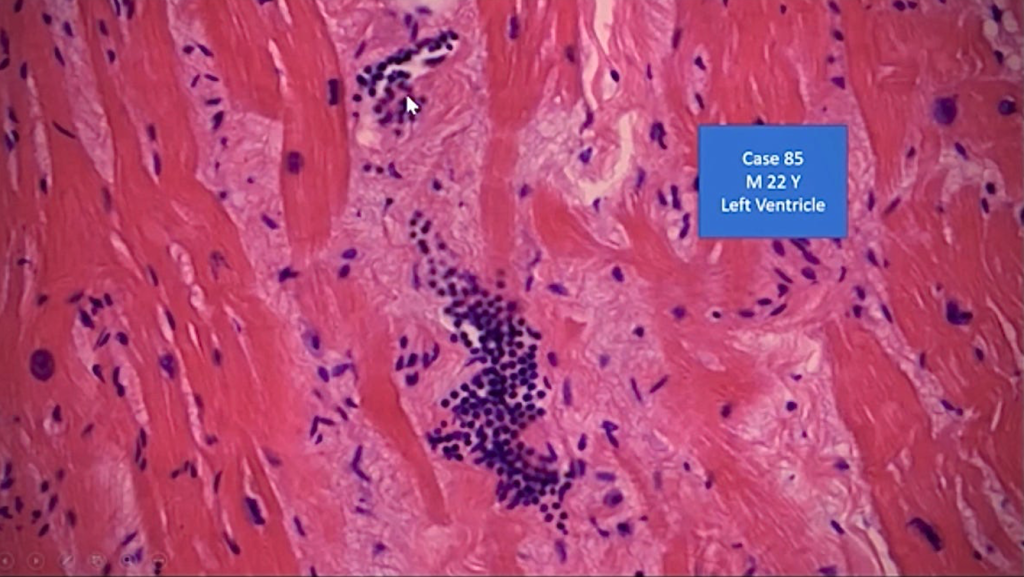
Before he died, Dr. Burkhardt presented one of the few, perhaps only, cases of autopsy after one year in a Pfizer BNT162b2 myocardial and aorta injured 22-year-old male athlete who committed suicide because of his medical condition.
This case was presented to the Canadian COVID Care Alliance (https://rumble.com/user/CanadianCovidCareAlliance) shortly before Dr. Burkhardt’s death on May 30, 2023.
https://rumble.com/v2jbj16-arne-burkhardt-presentation-to-the-ccca.html
The inflamed and necrotic (dead) muscle seen here is replaced by extensive scar tissue that is almost full thickness across the wall of the heart (left, lower quadrant extending across to the right side).
Scar tissue replacement of normal cardiac muscle makes the heart stiffer with compromised contractility (decreasing ejection fraction). If this process affects the electrical conduction system, an irregularly beating heart (cardiac arrhythmia) can result.
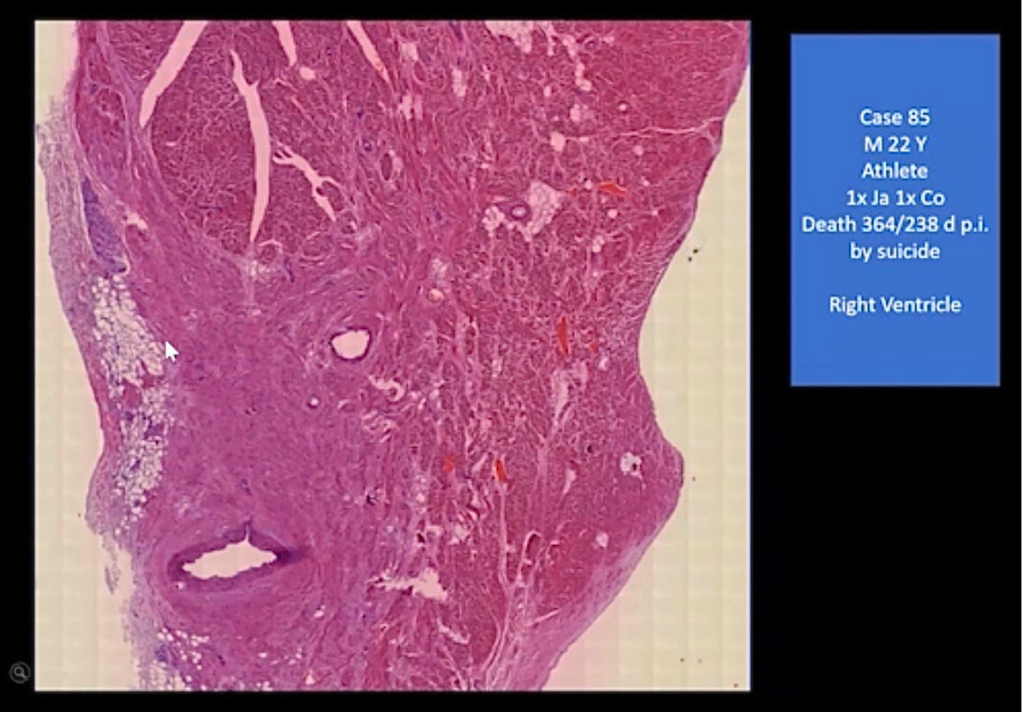
The section below illustrates some residual normal muscle in a matrix of rigid fibrous tissue that has replaced the necrotic muscle. There is a dense collection of lymphocytes with ongoing inflammation at 12 months post-injection.
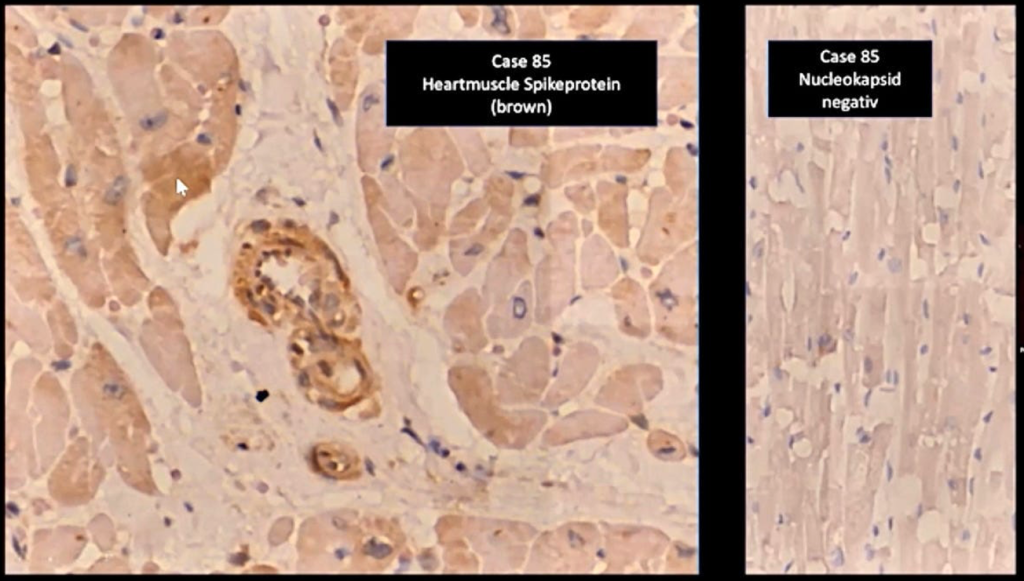
Dr. Burkhardt verified the cause of the diseased myocardium using one stain that is positive for spike from either the drug or the virus and a second that is positive only for cases caused by the virus. A year after injection, there is still spike protein in the heart, but there is no evidence that this heart was damaged by COVID.
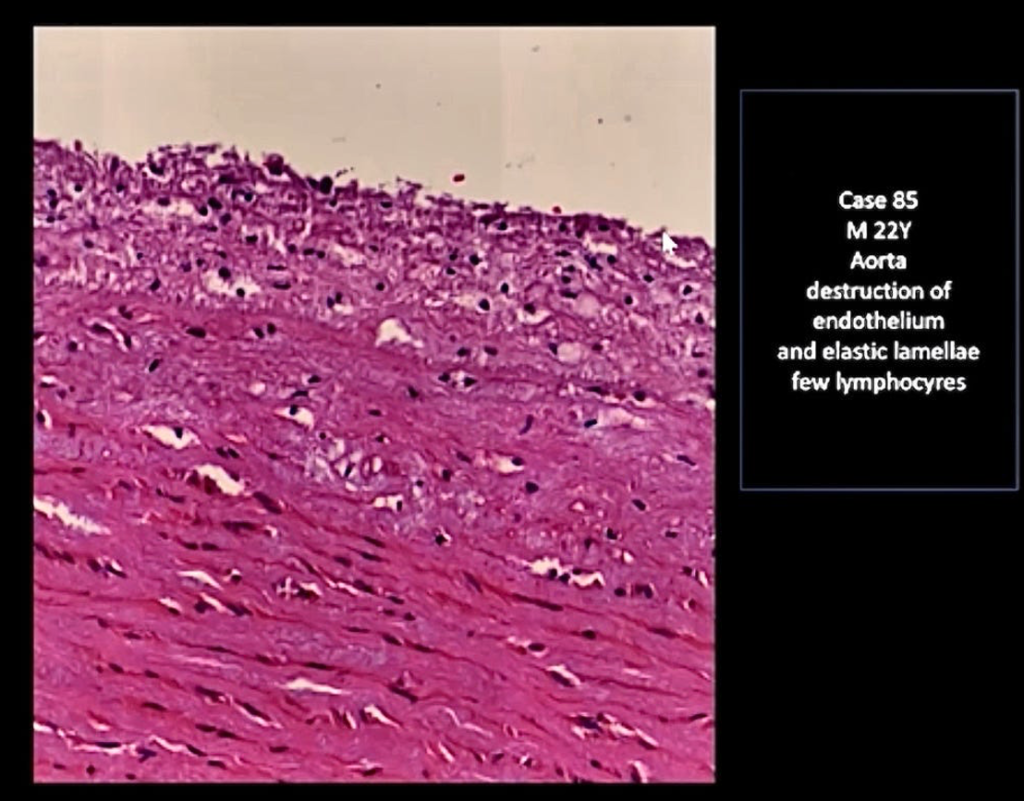
This unfortunate young man also had disruption of the muscular wall of his aorta that is forming an aneurysm as the inner layer of the aorta splits from the outer layer (below). Rupture of an aneurysm of the aorta can be rapidly fatal.
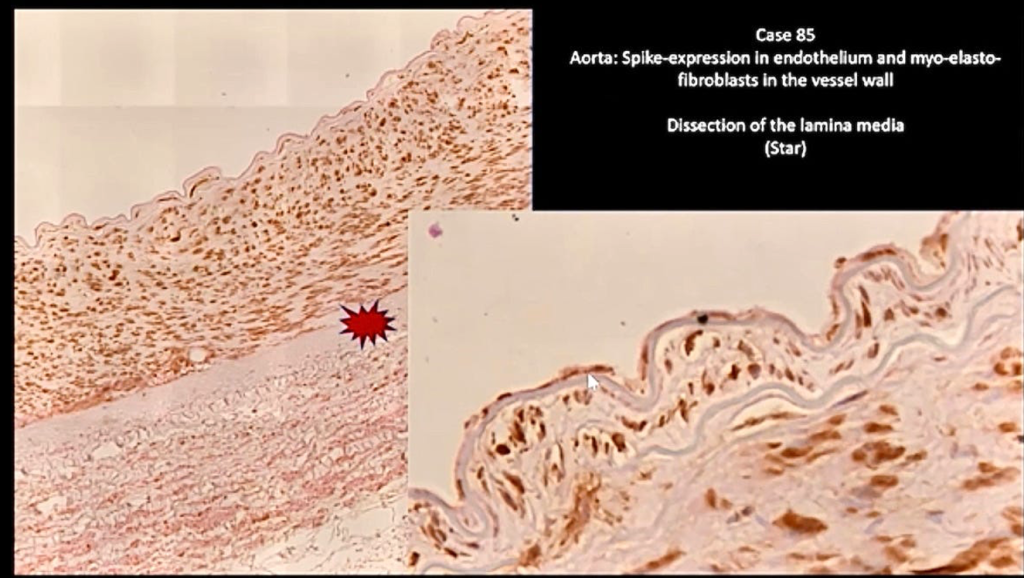
Spike proteins were designed to attach to a specific (ACE2) receptor on cells lining the inner wall of blood vessels called the endothelium. The slide below shows destruction of the endothelium in the aorta of the young athlete.
At this stage there is limited knowledge regarding the long term prognosis of CoVax (i.e., LNP/mRNA) heart disease in a specific sense. CoVax myocarditis may behave differently than other types of myocarditis.
This case illustrates the tragic consequences of cutting corners and making assumptions instead of making proper science. Pfizer Confidential Document 2.4 provides the assumption made about proteins expressed by the RNA in BNT162b2.
- “The protein encoded by the RNA in BNT162b2 is expected to be proteolytically degraded like other endogenous proteins. RNA is degraded by cellular RNases and subjected to nucleic acid metabolism. Nucleotide metabolism occurs continuously within the cell, with the nucleoside being degraded to waste products and excreted or recycled for nucleotide synthesis. Therefore, no RNA or protein metabolism or excretion studies will be conducted.” (p. 20, ¶3)
Sadly, they simply skipped this piece of work. And at least 15 others. See the review below of the Pfizer Pre-Clinical (“Nonclinical”) Studies Confidential Document 2.4 to see the other 15 areas that were not studies.
https://dailyclout.io/wp-content/uploads/Bnt162b2_Nonclinical_Overview.pdf
From Australia:
- Government Hearing: https://amgreatness.com/2023/08/04/pfizer-and-moderna-reps-put-on-the-hot-seat-in-fiery-senate-hearing-in-australia/
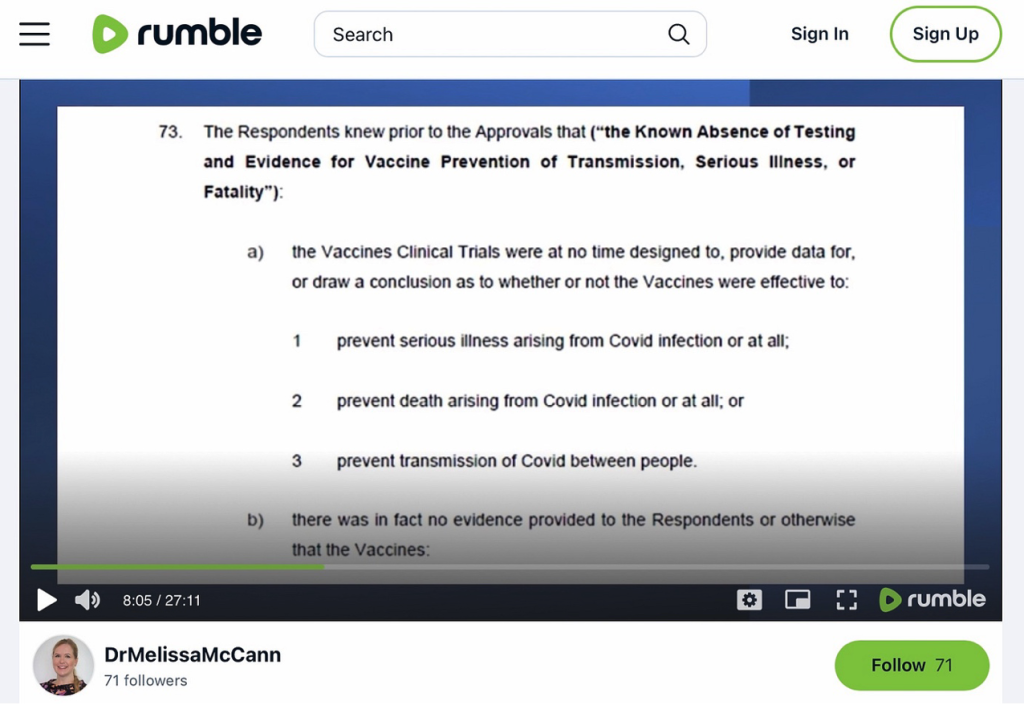
“The Republican-led U.S. House Select Subcommittee on the Coronavirus Pandemic has not yet called any witnesses from Pfizer, Moderna, Johnson and Johnson, the CDC, FDA, Anthony Fauci, or Francis Collins to appear before the committee and has shown no interest in investigating the fraud that allegedly took place in the COVID vax clinical trials.”
Class action lawsuit: https://rumble.com/v348nkr-covid-vaccine-injury-class-action.html
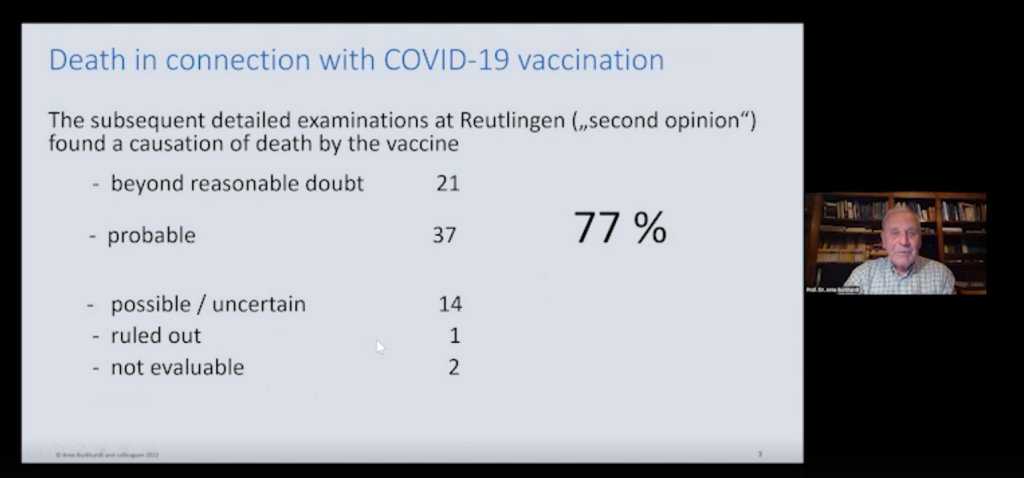
From Germany:
From All Over:
- “RETIRED SUDDENLY – NFL Players and International soccer players injured after taking COVID-19 vaccines – pericarditis, arrhythmia, ‘heart conditions’, blood clots in legs & lungs – 12 recent stories!” by William Makis, MD
- “Bronco KJ Hamler ‘steps back’; LSU coach Jimmy Lindsey ‘steps away’; Bears’ Steve McMichael in ICU; ex-Buckeye Drue Chrisman in hospital; Sooners coach Brent Venables’ wife has breast cancer” by Mark Crispin Miller
Conclusions:
Heart disease following injection of COVID-19 mRNA “vaccine” products is:
- Not rare.
- Not temporary.
- Not mild.
It is past time to seriously study this potentially catastrophic health problem, define its dimensions and severity, and then develop treatments to preserve life and function.



No comments:
Post a Comment