
mRNA Vaccines are “Vaccines”
Like it or not, mRNA vaccines are no less a vaccine than other vaccines
For the countless people who send me friendly messages like “STOP CALLING THEM A F---ING VACCINE” with regard to Pfizer and Moderna mRNA Covid-19 vaccines, I have some bad news: these Covid-19 vaccines are “vaccines.”
These messages, no doubt, arise from a desire to hold onto dogmatic beliefs about vaccines in general by claiming that mRNA Covid-19 vaccines are not “vaccines.” That “real” vaccines are different. Better. The reality, however, is that these vaccines are as much “vaccines” as any other vaccine.
Let’s go through the commonly cited reasons for claiming that mRNA vaccines are not vaccines made by those wanting to hold onto their beliefs about other vaccines.
mRNA Vaccines do not prevent infection and transmission!
Many point to the fact that mRNA vaccines do not prevent infection and transmission to argue they are not vaccines.
If the fact that a vaccine cannot prevent infection and transmission precluded it from being a “vaccine,” then numerous “traditional” vaccines cannot be considered “vaccines.”
For example, the pertussis vaccine, often used as the benchmark vaccine to assess overall community uptake of vaccines, would no longer be considered a vaccine because it does not prevent infection and transmission.
If you didn’t already know this, don’t take my word for it. Here is a quote from a recent consensus paper from 16 scientists, considered the world’s leading pertussis “experts” (many of whom receive funding from pharma companies that sell pertussis vaccines), and the World Association of Infectious Disease:
aPV pertussis vaccines do not prevent colonization. Consequently, they do not reduce the circulation of B. pertussis and do not exert any herd immunity effect.
(Note that aPV, acellular pertussis vaccine, is the exclusive pertussis vaccine used for decades in the United States and other developed countries.)
So, let’s read the bold portion above again: “aPV pertussis vaccines do not prevent colonization” and they “do not exert any herd immunity effect.” The paper even admits that the lack “of mucosal immune responses after aPV administration favorinfection, persistent colonization, and transmission of the pathogen.”
If preventing infection and transmission is necessary to call a product a vaccine, then pertussis vaccine cannot be called a vaccine.
Diphtheria and tetanus vaccines, too, would no longer be vaccines. These toxoid vaccines only generate antibodies to a toxin sometimes released by these bacteria; they do not generate immunity to diphtheria or tetanus bacteria themselves. Hence, as explained in the American Journal of Diseases in Children, “Diphtheria toxoid helps prevent symptomatic disease but does not prevent the carrier state nor stop the spread of infection.” That is because vaccinated individuals can still become infected because they only have antibodies to the toxin sometimes released by these bacteria; they do not have antibodies to the bacteria themselves.
Even if the tetanus vaccine did generate immunity to the tetanus bacteria itself, which it doesn’t, it cannot prevent transmission and has nothing to do with so-called “community immunity” because, as explained by the CDC, tetanus “is not contagious from person-to-person.”
So, again, if preventing infection and transmission is necessary to call a product a vaccine, neither tetanus vaccine nor diphtheria vaccine are vaccines.
And hold tight for the final example. It may invoke severe cognitive dissonance for some. The polio vaccine. Most developed countries ceased using oral polio vaccine (OPV) decades ago because this vaccine could cause paralysis, and instead have exclusively used inactivated polio vaccine (IPV), which does not prevent infection and transmission.
This is because polio multiplies and spreads from fecal to oral contamination (meaning poop to mouth). Yet, IPV creates immunity in the blood (IgG antibodies), not the intestinal tract (IgA antibodies); hence, vaccinated individuals can still become infected and transmit polio. It creates antibodies intended to neutralize the polio virus in the bloodstream before it can reach the spinal column, but it doesn’t neutralize the virus from multiplying in the intestinal tract and shedding in the feces.
Sound untrue? Feel free to argue with the WHO and CDC about it, whose global polio eradication initiative explains:
“when a person immunized with IPV is infected with wild poliovirus, the virus can still multiply inside the intestines and be shed in the faeces, risking continued circulation” and that “as IPV does not stop transmission of the virus, OPV is used wherever a polio outbreak needs to be contained, even in countries which rely exclusively on IPV for their routine immunization programme.”
There you have it, from the horse’s mouth. So, again, if preventing infection and transmission is necessary to call a product a vaccine, then the polio vaccine used in developed countries -- originally developed by Jonas Salk and the vaccine often used as the archetypal example of a “vaccine” -- would also not be a vaccine.
Bottom line: if mRNA vaccines cannot be called “vaccines” because they do not prevent infection and transmission, then a large proportion of the current vaccines can no longer be called “vaccines,” including pertussis, tetanus, diphtheria, and polio vaccines.
The definition of “vaccines” changed!
The next argument I have heard repeatedly is that the definition of “vaccines” changed to accommodate mRNA vaccines.
In reality, mRNA vaccines fit well into the CDC’s definition of “vaccines” in its “Vaccines & Immunizations Glossary” from the pre-Covid era. Here is the definition of “vaccine” and “immunity” from the CDC’s Vaccine & Immunization Glossary from February 2019:
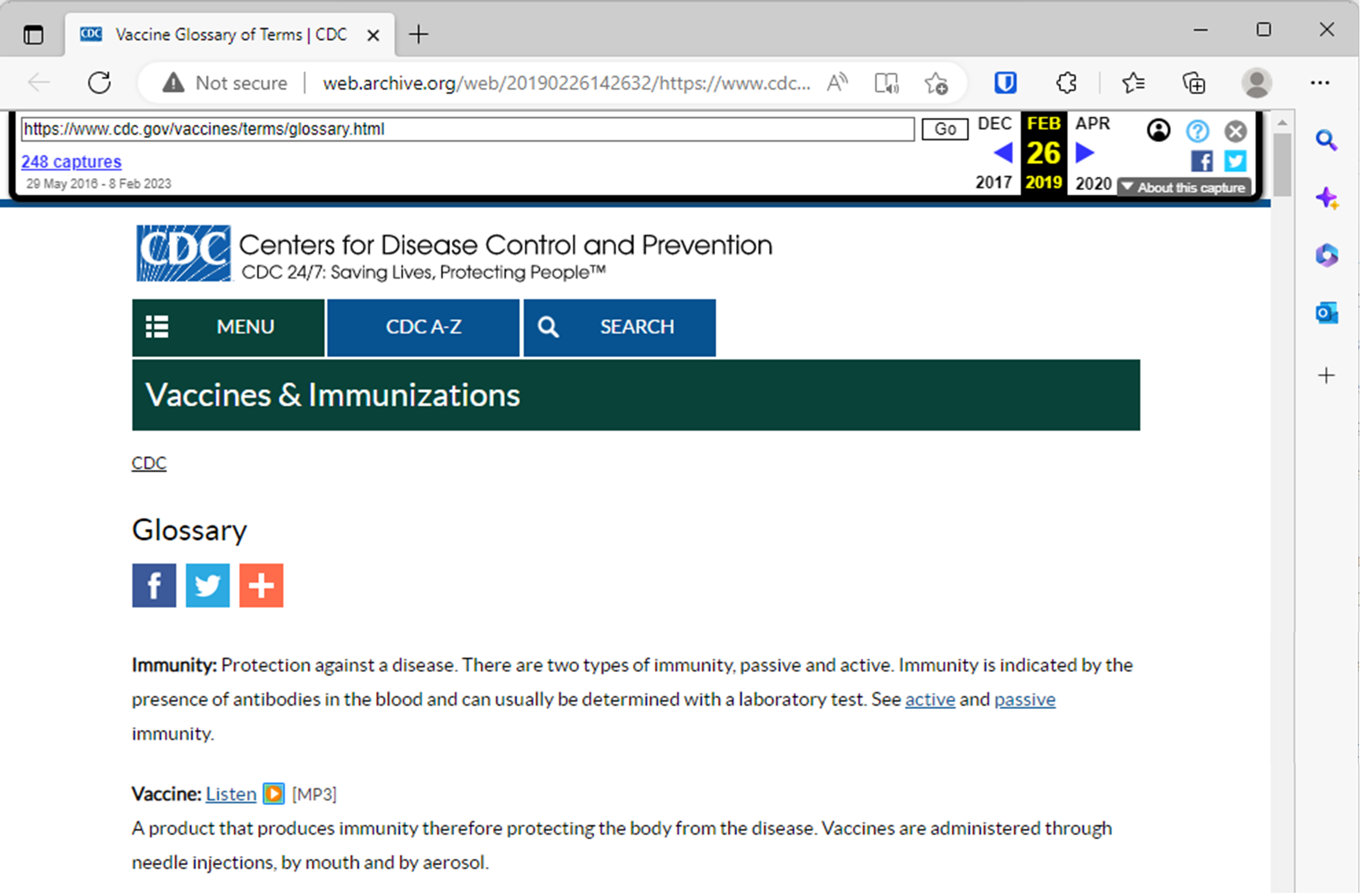
As you can clearly read above, “vaccine” was defined as a “product that produces immunity,” and the term “immunity” is determined by “the presence of antibodies in the blood.” The mRNA Covid vaccines fit neatly into this definition since they generate antibodies in the blood for the virus that causes Covid-19 and appears to provide at least some protection from some symptoms of Covid-19 for a very limited time after injection.
This CDC Glossary of terms for “Vaccines & Immunizations” has been my go-to glossary for over half a decade when quoting the CDC’s definition of vaccine-related terms (for example, see page 100 of this December 2019 complaint) and the pre-Covid definition of “vaccine” and “immunity” is the same for as far back as the WayBackMachine has copies of this page, back to May 29, 2016.
(There is apparently another pre-Covid era definition of “Vaccine” on a different CDC webpage, titled “Immunization: The Basics.” That page defined “Vaccine” as “A product that stimulates a person’s immune system to produce immunity to a specific disease” and defined “Immunity” as “[i]f you are immune to a disease, you can be exposed to it without becoming infected.” But this definition was clearly outdated decades before 2020 because, under that plainly long-outdated definition, tetanus vaccine, pertussis vaccine, inactivated polio vaccine, and numerous other vaccines would not qualify as a “vaccine” since none prevent infection, as discussed above.)
Bottom line, mRNA vaccines fall squarely into the definition of “vaccine” used by the CDC in its glossary of terms for “Vaccines & Immunizations” prior to the Covid-19 era.
But all other vaccines work the same way, and this one is different!
The next argument some make is that the mRNA Covid-19 vaccines seek to generate immunity in a different way than prior vaccines do. This presumes that the way in which all prior vaccines generated immunity is nearly identical. Nothing could be further from the truth.
Almost all vaccines are different, often very different, technologically, mechanistically, etc. But they all have one thing in common: they artificially stimulate the immune system to generate an immune response. That is equally true of the mRNA vaccines.
For example, hepatitis b vaccines are made from recombinant DNA technology. This is DNA technology by which they pluck out the plasmid (a small DNA molecule) from a bacterium, slice out a section to insert an antigen from the hepatitis b virus, then insert that Frankenstein DNA into a yeast cell and then into fermentation tanks. The resulting brew results in a substance not available anywhere in nature but injected into humans. Mostly newborn humans.
Then there are attenuated vaccines. Rubella vaccine, for example, is passaged 25 times through the cultured cell line of aborted fetal tissue. The resulting Frankenstein virus, again nowhere to be found in nature, is injected deep into muscle tissue and takes over the cellular machinery of the cells it enters. You read that correctly. Just like mRNA vaccines that take over the cellar machinery of ribosomes to produce proteins, attenuated Frankenstein rubella viruses take over the cellular machinery of the cell to replicate this Frankenstein virus.
(And as a bonus, as explained by the inventor of the rubella vaccine, each dose of rubella vaccine contains a vast amount of human DNA and cellular debris from the aborted fetal cell line that are then injected along with the Frankenstein rubella virus.)
Next are toxoid vaccines, such as the ones for tetanus and diphtheria, discussed above. These vaccines take the most dangerous part of these bacteria, a toxin they each release, and treat them with formaldehyde. Those formaldehyde-treated toxins are then injected into the body. Sounds very much like the claim that the Covid-19 mRNA vaccines cause a toxin – spike protein – to end up in the body.
The point is that vastly different technologies are used to make various vaccines and arbitrary lines could be drawn to render any number of vaccines no longer “vaccines” based on the technology utilized. That would produce nonsensical results in defining what is a vaccine. There is a common denominator between all vaccines and it is not what technology is utilized. The common denominator is that they all artificially stimulate the immune system in the attempt to generate antibodies to a disease. Most are injected deep into muscle tissue, an unnatural route of exposure, and cause a sustained immune response.
(To be clear, I am not saying that mRNA vaccines, like many other vaccines, should not also be considered gene-based therapy. They should! All vaccines, in fact, are considered “both a drug and a biological product” under the applicable regulations, but are nonetheless licensed through the biologic division of the FDA, regardless of whether it is a recombinant DNA vaccine, mRNA vaccine, polysaccharide vaccine, conjugate vaccine, toxoid vaccine, viral vector vaccine, etc. Many of these should have also undergone the studies appropriate for gene-based therapies, drug therapies, etc., but that, again, doesn’t mean they are not vaccines. They are.)
It is also worth noting that every vaccine causes a cascade of events between injection and generation of antibodies. Differences in this cascade of events are not material to the definition of “vaccine” as discussed above. It is also unclear why some think that injecting mRNA – which enters muscle cells, takes over cellular machinery to produce spike protein, and expresses this protein manufactured in the cell that then gets picked up by the immune system to create an antibody – is any less a vaccine than, say, a measles vaccine – which causes a Frankenstein man-made version of the measles virus to enter muscle cells, take over the cells machinery to replicate itself, and expresses a protein manufactured in the cell that then gets picked up by the immune system to create an antibody.
The steps between injection and antibody production are even more complicated for other vaccines. The point is that while the process and steps between injection and antibody production vary widely for each vaccine, and the technology deployed varies widely between vaccines, the result is the intended production of antibodies. That is what makes mRNA vaccines and all other vaccines fit neatly into the definition of “vaccines.”
They were rushed!
The next stop on the “mRNA vaccines are not vaccines!” train is to claim that they were rushed, “unlike other vaccines.”
That is probably the most nonsensical argument of all. The technology used to create mRNA vaccines took decades to develop, just like the technology used for various other vaccines. The appropriate and critical question is not how long it took to develop the technology but rather how robust the clinical trials were that tested each vaccine’s safety and efficacy in humans.
The clinical trials for Pfizer and ModernaCovid-19 vaccines each enrolled at least 30,000 people, reviewed safety for at least six months, and had a placebo control group for at least two months on average.
In contrast, most childhood vaccines had only days or weeks of safety review; typically far, far less than 30,000 participants; and virtually never had a placebo control. As an example, let’s use the very first vaccine on the CDC’s childhood schedule – the hepatitis b vaccine given on the first day of life:
The safety review in the clinical trial relied upon to license this vaccine is similar to that of many other vaccines on the childhood schedule. In a word: useless. Now let me earn the use of that adjective.
There are only two brands of hepatitis b vaccines that are given to babies on the first day of life, Recombivax HB and Engerix B. Here is a summary of the clinical trial relied upon to license Recombivax HB for babies and children directly from the official FDA documentation:
So, 147 children were injected with 5 days of safety monitoring after injection. The clinical trial for Engerix B (see page 6), the other hepatitis b vaccine given to babies, only had 4 days of safety monitoring after vaccination.
This seems so unbelievable that, on behalf of Informed Consent Action Network (ICAN), my firm sent a Freedom of Information Act request to the FDA demanding copies of the clinical trial reports submitted to the FDA to license Recombivax HB, and you can see for yourself it was indeed five days of safety monitoring after each shot given to babies and children! For Engerix B we requestedthat the FDA only produce clinical trial reports that reviewed safety for more than a week and after 3 ½ years, the FDA has still never been able to produce a single such study!
(See, also, this petition, submitted on behalf of ICAN to the FDA, demanding that it require proper clinical trials of these products or rescind their licensure until these are completed; the six month deadline for the FDA to respond to this petition has long passed because, no doubt, they cannot possibly justify what the agency did.)
And if you are thinking, as I did, that maybe, just maybe, a clinical trial or some other large, robust safety assessment occurred after licensure (even though it would be condemned by the medical community as unethical – to withhold an “effective” vaccine from children in the control group), you would be wrong. Read this exchange between ICAN and the U.S. Dep’t of Health & Human Services (HHS, which includes FDA, CDC, and NIH) for yourself.
You will also see in this formal exchangebetween ICAN and HHS the details of the safety review period and controls used in the clinical trial for each of the vaccines given to infants.
Once you do, you will realize that if you were going to take a vaccine based on the robustness of its clinical trial, you would take an mRNA vaccine before any other vaccine on the childhood schedule!
Bottom line: as you can now see, the purported “rushed” clinical trials for the mRNA vaccines do not set them apart from other vaccines. And, if the robustness of a clinical trial makes the product more worthy of the title “vaccine,” then mRNA vaccines have more than earned this title.
You can’t sue Pfizer and Moderna for harms!
Finally, a few people have sought to distinguish mRNA vaccines by explaining that you cannot sue Pfizer and Moderna for harms caused by their mRNA vaccines. But that is also true for all the vaccines on the CDC’s childhood vaccine schedule – you also effectively cannot sue the pharma companies selling these vaccines for harms.
The current laws immunizing pharmaceutical companies from liability differ, but all vaccines recommended for routine use in children enjoy liability protection just as mRNA vaccines do. Pharma companies enjoy financial immunity for harm for Covid-19 vaccine injuries pursuant to the PREP Act, and they enjoy financial immunity for harm for childhood vaccines pursuant to the National Childhood Vaccine Injury Act of 1986.
The 1986 law was enacted because there was only one manufacturer left for each of the only three routine vaccines at that time, and the harms they caused created financial liability exceeding their revenue. Instead of letting the normal market forces drive these companies to make better and safer products, Congress just gave them financial immunity for the injuries so they could keep selling their harmful vaccines with impunity. Incredibly, it also gave them financial immunity for any future childhood vaccines.
Bottom line: pharma companies selling Covid-19 vaccines or childhood vaccines can equally harm you with impunity.
There is a critical difference between the mRNA vaccines and other vaccines
The real difference between all the previously-existing vaccines and the mRNA vaccines is that these new vaccines were given to over 260 million Americans in a short time period, and there has been an atypical amount of public scrutiny of this product. The harms they caused are, therefore, hard to hide given the clear “before” and “after” amongst the world’s population.
In contrast, virtually all childhood vaccines were rolled out slowly over decades and were given to a narrow birth cohort each year, with uptake in each birth cohort only fractionally increasing. Therefore, two decades after a childhood vaccine is introduced, we still typically have only those 20 years old and younger who received that shot, and it took those twenty years to get even a portion of those people under aged 20 vaccinated. During that period, health issues that may arise following vaccination would recede into the background rates and become the new health “normal.”
For example, had the Covid-19 vaccine been rolled out like most childhood vaccines, it would have taken decades to get only a fraction of the population vaccinated. If rates of myocarditis increased steadily during that period, by the time anyone noticed, there is likely nil chance that “health” authorities would ever attribute it to the Covid-19 vaccines. That rate of myocarditis would just become the new health “normal.”
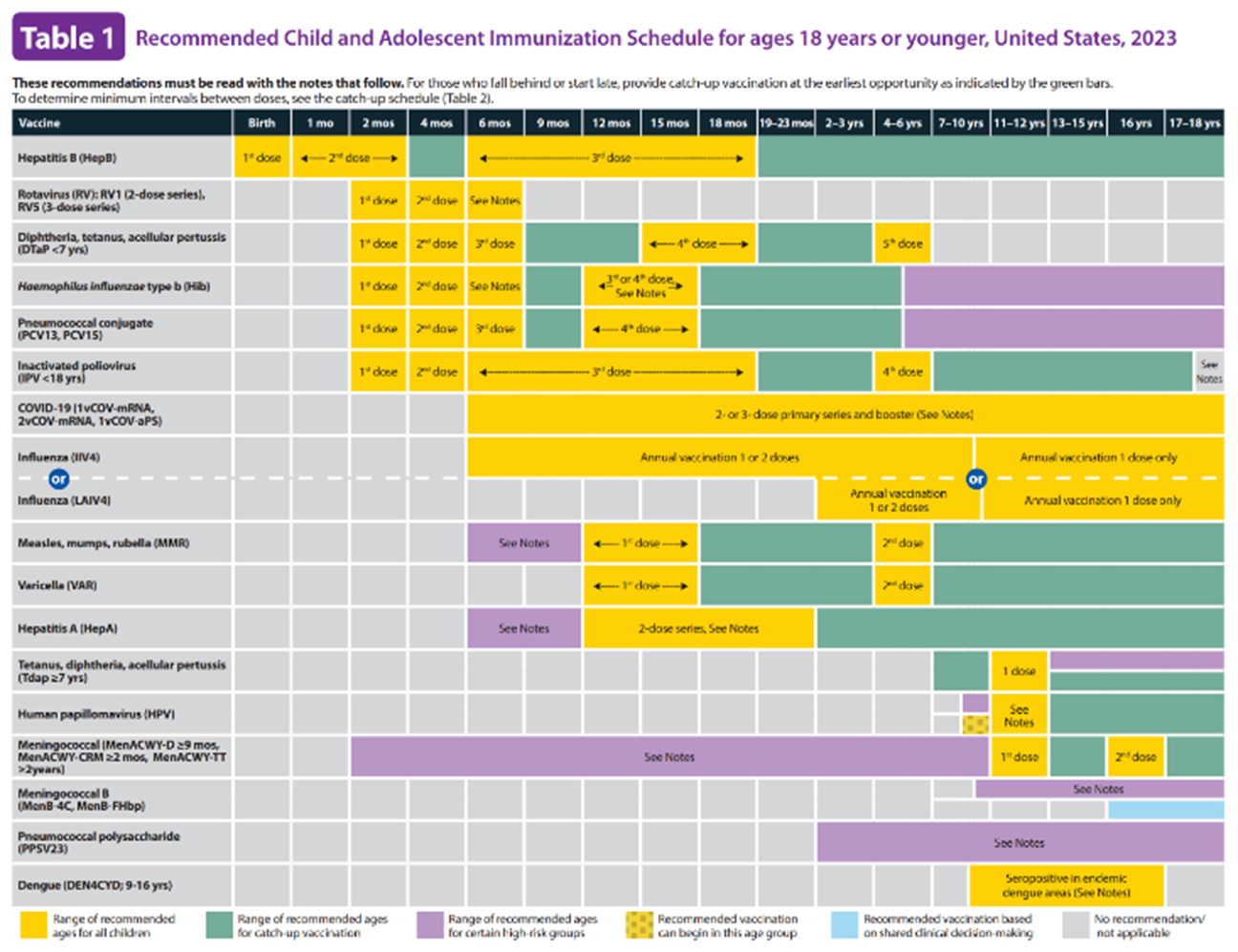
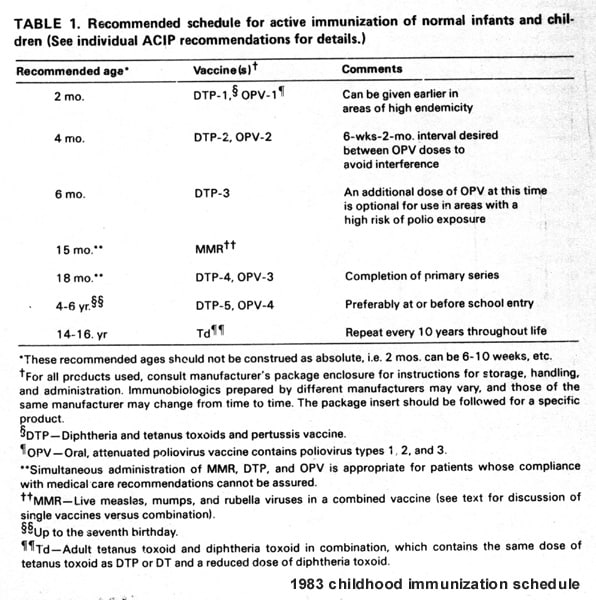
Consider that the rate of chronic health issues among children is reported to have gone from around 11% of children in 1986 (when there were three routine childhood vaccines) to approximately 50% now (with seventeen vaccines on the childhood vaccination schedule). This image is the current schedule for babies up to just 7 months of age:
To what degree did childhood vaccines cause or contribute to this rise in chronic health issues? I don’t know the answer to that, but I do know it has not been adequately studied despite the fact that many of the chronic health issues exploding in children since 1986 are immune or immune-mediated issues. Yet, despite this lack of study, federal “health” authorities will assure you these vaccines are “safe.”
The point is that any potential adverse health effects of Covid-19 vaccines have been sharp and pronounced because, instead of vaccinating maybe less than 1% of the population every year (often infants who cannot adequately communicate reactions), around 80% of the United States population (mostly adults) was rapidly vaccinated with a Covid-19 vaccine. The before and after health effects of the Covid-19 vaccines (despite the best efforts of “health” authorities) are hard to hide. The harms caused did not have time to recede into the background rate.
And who suffered these harms? Babies who can’t talk? No. It was adults who can clearly articulate what happened to them. That type of experience causes tension between the oft-repeated claim of safety from public “health” officials and people’s personal experiences.
This results, for some, in cognitive dissonance, which, in turn, causes many to want to compartmentalize what they see occurring with Covid-19 vaccines. “It’s just the Covid-19 vaccine – this one is different.” That is easier to accept than to understand that perhaps it’s not just the Covid-19 vaccine.
And just like the many brave doctors and scientists who are trying to raise the alarm about harms from Covid-19 vaccines, there have also been brave doctors and scientists who have tried to raise the alarm about serious harms caused by the hepatitis b vaccine and other vaccines. Those doctors were no less articulate, educated, or credentialed than those now blowing the whistle about Covid-19 vaccines. The difference is that those raising concerns about Covid-19 vaccines have at least half of the political media spectrum willing to give them airtime. If nothing else, they can write a Substack!
One final difference is that most so-called “vaccine-preventable diseases” are blamed for causing dozens or a few hundred deaths per year in the United States in the years prior to a vaccine being introduced. The great killer, measles, for example, according to the CDC, caused around 400 deaths (see page 158) in the United States in the years before the first vaccine in 1963 – that amounts to 1 in 500,000 Americans during a time when measles was endemic and infected nearly everyone. It was also when parts of the United States still had the type of living conditions that made measles dangerous.
In contrast, Covid-19 is blamed for killing hundreds of thousands of Americans in 2020 before the a vaccine. According to the CDC all-cause mortality data (meaning all deaths), there was indeed an increase of 588,167 total deaths in 2020 (total of 3,433,986 deaths) versus 2019 (total of 2,845,819 deaths). So, something was killing a lot more people in 2020 and, even accounting for improper medical treatments, lockdowns, etc., presumably some portion of these deaths was from Covid-19. It is, therefore, unlike virtually any other pathogen for which we vaccinate (as most had even less deaths per year in the United States than measles vaccine prior to vaccination -- and again, during a time when clean water, sanitation, acute medical care, etc., were far less advanced).
This mean that in order to have a proper risk/benefit ratio, the safety profile of childhood vaccines needed to be hundreds of times safer than Covid-19 vaccines. Yet, the clinical trials for Covid-19 vaccines (conducted during a declared emergency and mostly intended for adults) were incredibly more robust than the trials for childhood vaccines.
A prediction
I predict that in the coming years, when memories start to blur, the CDC and FDA will declare (as it has done with certain other vaccines) that Covid-19 was brought to heel because of the Covid-19 vaccines.
The CDC has already published numerous “studies” in its non-peer-reviewed “science” journal, the MMWR, to support this policy position. And this should not be surprising because, as the CDC explains: “By the time a report appears in MMWR, it reflects, or is consistent with, CDC policy.”
I am sure for anyone paying attention right now this seems like it would be an incredible claim. But just give it time. Consider that if Fauci said it right now, there is a significant percent of Americans who would accept it as true.
As the years pass, a combination of apathy and blurry memories will make that percentage higher. Keep repeating it was the Covid-19 vaccines that “saved us” for a few decades, and put it on the CDC website, and repeated it the medical literature, and it will just be the “anti-science” crowd that thinks otherwise down the line.
At that point, there will likely also be nobody or almost nobody left saying Covid-19 vaccine is not a “vaccine.”
What truly makes a Covid mRNA vaccine a vaccine, the solution to its harms, & final notes
I want to thank everyone for the many gentle and friendly reminders that mRNA vaccines are not vaccines, but I just cannot agree. Based on my experience having heavily litigated vaccine-related issues, deposed world-leading vaccinologists, and dealt with vaccine matters for nearly a decade, I see very little difference between mRNA vaccines and all other vaccines.
The main difference may be the number of people who simply refuse to admit that mRNA vaccines, like DNA vaccines, viral vector vaccines, etc., are all vaccines that fall into the same economic and regulatory model that permits pharma to harm people with impunity with these products.
(Behind the paywall below: What truly makes mRNA vaccines and all other vaccines the same; the solution to the harms from the Covid-19 vaccine; and a few personal notes – enjoy!)
What truly makes mRNA vaccines the same as all vaccines, including the ones mandated for school children, is their economic and regulatory framework. They were developed and trialed by pharma companies that knew beforehand that they would not be liable for injuries and that HHS, FDA, CDC, and NIH would promote their products, push for mandates of their products, and literally defend (in the VICPor CICP) against any claim they cause injury.
The same paradigm — wherein the market forces that assure product safety have been neutered, and the federal regulators responsible for safety do not fulfill that duty because it conflicts with their duty to get them in the arm of every adult and child — exists regarding virtually every vaccine on the CDC’s childhood and adult vaccine schedules.
It is time to shift that paradigm. We need to let market forces again assure the safety of all vaccines by permitting injured individuals to sue the pharma companies selling these products.
This will drive pharma companies to conduct careful clinical trials to ensure the product, once licensed, won’t create a financial liability. It will drive pharma to timely address safety issues after licensure to avoid liability. It will align their profit motive with an interest in improving safety.
As things stand now, taking any of the foregoing steps to assure safety only reduces the manufacturer’s potential for profits. Without financial liability for harm, their only incentive regarding safety is not to let it be a barrier to getting a product to market. Any pharma company that let’s safety slow down the path to licensure will lose the profit race for developing a new vaccine.
For example, this chart does a good job of showing the reward Pfizer reaped for being the first to market with a Covid-19 vaccine:

And as for the FDA, it needs to stop promoting vaccines! Its job is to critically and objectively review the data submitted by the pharma company to license a vaccine. It cannot do that if it acts as a cheerleader for the vaccine. Yet, here is the homepage of the FDA website for the bivalent booster that is not yet even licensed:
And here is a promotional ad by Dr. Peter Marks, head of the FDA’s vaccine division, who will effectively decide whether to license the bivalent Covid-19 vaccine (which is again not licensed but currently only authorized for emergency use):

How in the world can Dr. Marks and the FDA be critical and objective in deciding whether to license a product if they are already pushing every American to take it?! That would require them to admit—“Oops, remember that product we encouraged you to get? Yeah, it’s actually not safe enough for licensure.”
As for the CDC, the ultimate cheerleader for vaccines, it cannot possibly be responsible for safety (yet, it is – see VAERS and v-safe, etc.). That critical responsibility must be in the hands of a completely different agency independent of the current federal “health” department structure.
For example, the promotion and safety function for transportation was split between the Department of Transportation and the National Transportation Safety Board because the duties to promote an industry and assure its safety are inherently at odds. Likewise, there needs to be an entirely independent federal board for vaccine safety because, as it stands now, the same federal agency is conflicted between both promoting vaccines and regulating/assuring the safety of vaccines.
But it would be naïve to think these common sense requests (to assure the safety of a medical product typically given to babies!) will be implemented easily or ever. Pharma is reported to have far more than 1,000 lobbyists in Washington D.C., and is constantly pushing to increase profit margins. As for “health” authorities, they view injecting everyone as a religious calling. It is about vaccination rates. Not health.
But there is some good news.
The good news is that you don’t need to fight to fix this entire broken system to protect yourself and your family from a medical product you deem more harmful than beneficial. Instead, you need only fight for something far narrower: the right to informed consent – the ability to say “no” without penalty. Meaning, you need only fight to assure nobody is mandated to receive a medical product, or if there is a mandate, there is a check-the-box no-questions-asked exemption. That is the simple solution.
It also aligns with the core value of individual and civil rights to, among others, informed consent and bodily integrity. The lack of respect for individual and civil rights has wrought more harm on humanity than anything else. The American experiment was a rebellion against the idea that you must cede your rights to some overseers who knows better and will make decisions on your behalf.
To that end, as I often repeat, please send the following proposed legislation to your legislative representatives:
“No law may require or coerce a person to receive or use a medical product, or impose a penalty or deprive a benefit for refusing a medical product or refusing to disclose whether a person has received a medical product.”
Medical freedom is freedom. If you cannot get a job, go to school, or otherwise participate in civil society because you refuse a medical product, then what good are your rights if you can only exercise them at home by yourself? That is why medical freedom is a fundamental right that must be permanently fixed into the law of every civilized nation.
We are, as provided in the Declaration of Independence, indeed “endowed by their Creator with certain unalienable Rights” and to safeguard those rights “we mutually pledge to each other our Lives, our Fortunes, and our sacred Honor.” We must never yield to the tyranny of permitting others to dictate what can or must be placed, administered, or injected onto or into our bodies. For once that right is ceded, none truly remain.




{kind=link}
No comments:
Post a Comment