
We Now Have Proof The COVID Vaccines Damage Cognition
Superb and all-important article by A Midwestern Doctor. Examining the causes and treatments of the common neurological injuries caused by vaccination.
BS”D

Two weeks ago, the first study, published in Nature, found that COVID vaccination resulted in a 68% increase in depression, a 44% increase in anxiety, dissociative, stress-related, and somatoform disorders, a 93.4% increase in sleep disorders, a 77% decrease in schizophrenia, and a 32.8% decrease in bipolar disorder.
Around the same time (three weeks ago) another article was published in a mainstream journal (or to be more exact “accepted for publication”). It analyzed individuals over 65 and found COVID vaccination increased the risk of mild cognitive impairment 138% and the risk of Alzheimer’s by 23%.
To put this in context, given that America spends over 300 billion dollars per year on Alzheimer’s disease, this single datapoint effectively means that the COVID vaccines cost the United States around 100 billion dollars.
(The above increase was only from tracking patients for 3 months. Unfortunately it reflects just the tip of the iceberg, as dementia is progressive.)
This article is by A Midwestern Doctor
(Link to original below.)
Story at a Glance:
•Subtle and overt neurological injuries are one of the most common results of a pharmaceutical injury.
•The COVID-19 vaccines excel at causing damage to cognition, and many of us have noticed both subtle and over cognitive impairment following vaccination that relatively few people know how to address.
•For a long time, the hypothesis that the vaccines impaired cognition was “anecdotal” because it was based on individuals observing it in their peer group or patients.
•Recently large datasets emerged which show this phenomenon is very real and that the severe injuries we’ve seen from the vaccines (e.g., sudden death) are only the tip of the iceberg.
•In this article we will review the proof vaccine are doing this and explore the mechanisms which allow it to happen so we can better understand how to treat it.
When the COVID-19 vaccines were brought to market, due to their design I expected them to have safety issues, and I expected over the long term, a variety of chronic issues would be linked to them. This was because there were a variety of reasons to suspect they would cause autoimmune disorders, fertility issues and cancers—but for some reason (as shown by the Pfizer EMA leaks), the vaccines had been exempted from being appropriately tested for any of these issues prior to being given to humans.
Since all new drugs are required to receive that testing, I interpreted it to be a tacit admission it was known major issues would emerge in these areas, and that a decision was made that it was better to just not officially test any of them so there would be no data to show Pfizer “knew” the problems would develop and hence could claim plausible deniability. Sadly, since the time the vaccines entered the market, those three issues (especially autoimmunity) have become some of the most common severe events associated with the vaccines.
At the start of the vaccine rollout, there were four red flags to me:
•The early advertising campaigns for the vaccines mentioned that you would feel awful when you got the vaccine, but that was fine and a sign the vaccine was working. Even with vaccines that had a very high rate of adverse events (e.g., the HPV vaccine), I had never seen this messaging before. This signified it was likely the adverse event rate with the spike protein vaccines would be much higher than normal.
•Many of my colleagues who got the vaccine (since they were healthcare workers they were able to get it first) posted on social media about just how awful they felt after getting the vaccine. This was also something I had never seen with a previous vaccine. After some digging, I noticed those with the worse vaccine reactions typically had already had COVID and had their reaction was to the second shot rather than the first, signifying that some type of increased sensitization was occurring from repeated exposures to the spike protein. Likewise, the published clinical trial about Pfizer’s vaccine also showed adverse reactions were dramatically higher with the second rather than first shot.
•Once the vaccine became available to the general public, I immediately had patients start showing up with vaccine reactions, many of whom stated they received their flu shot each year and never had experienced something similar with a previous vaccination. One of the most concerning things were the pre-exacerbation of autoimmune diseases (e.g., spots in their body they previously would occasionally have arthritis in all felt like they were on fire). After I started looking into this I realized people were seeing between a 15-25% rate of new autoimmune disorders or exacerbations of existing autoimmune disorders developing after the vaccine a massive increase I had never seen any previous vaccine cause.
Note: this was demonstrated by a February 2022 Israeli survey which showed 3% of vaccine recipients experienced a new autoimmune disorder and that 24% experienced an exacerbation of a pre-existing one, a rheumatologic database published in the BMJ that found 4.4% of recipients experienced an exacerbation of a pre-existing autoimmune disease, and a survey by a private physician of 566 patientswhich found vaccination spiked their inflammatory markers, causing their five year risk of a heart attack to go from 11% to 25%.
•About a month after the vaccines were available to the public, I started having friends and patients share that they’d known someone who had unexpectedly died suddenly after receiving the vaccine (typically from a heart attack, stroke, or a sudden aggressive case of COVID-19).
This was also extremely concerning to me, because reactions to a toxin typically distribute on a bell curve, with the severe ones being much rarer than the moderate ones. This meant that if that many severe reactions were occurring, what I could already see was only the tip of the iceberg and far, far more less obvious reactions were going to be happening, to the point it was likely many people I knew would end up experiencing complications from the vaccine.
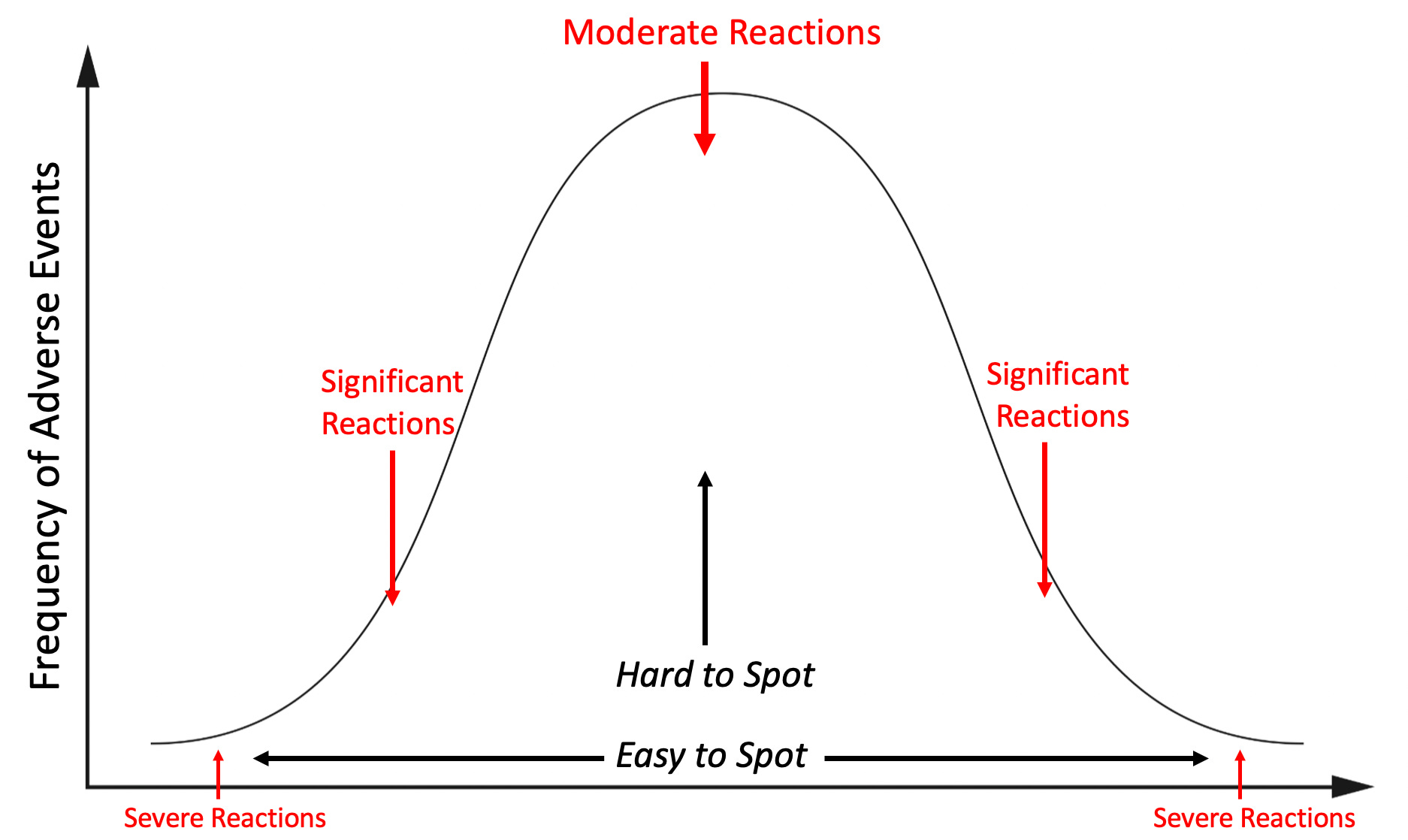
Note: the above graph is only illustrating one aspect of the picture as there will also be a much larger number of minor reactions, and even more invisible ones (e.g., a symptom occurs years down the road) or no reaction at all.
I tried to warn my colleagues about the dangers of this vaccine, but even when I pointed out Pfizer’s own trial admitted the vaccine was more likely to harm than help you, no one would listen to me. Not being sure what else to do, but not be willing to do nothing, I decided to start documenting all the severe reactions I came across so I could have some type of “proof” to show my colleagues.
This was something that was extremely important at the time since no one was willing to take on the personal risk of publishing something that went against the narrative (that vaccines were killing people) in the peer reviewed literature. Shortly after Steve Kirschkindly helped launched my Substack, I decided to post the log I’d put together, and since there was a critical need for that information (as many had seen the same things I’d observed but no one was reporting them), the post went viral and created much of the initial reader base that made my Substack possible.
It was immensely time consuming to do the project (especially the verification of each story that was reported to me), so I ended the project after a year. During that time, I came across 45 cases of either a death (these comprised the majority of the 45 cases), something I expected to be fatal later on (e.g., a metastatic cancer) or a permanent and total disability. Additionally, in line with the previously described bell curve, I also came across many more serious but not quite as severe injuries.
What I found remarkable about this was that through a passive reporting system in my own limited social network (I learned of these cases because people reached out to me or someone off-handedly shared them with me), I alone found enough cases of severe vaccine injuries to justify pulling the COVID-19 vaccines from the market, yet, our healthcare authorities, who had access to thousands of times as much data as I did chose to pretend nothing was happening. Furthermore, from my own dataset (due to it being large enough to contain all the common COVID vaccine injuries), I accurately predicted most of the vaccine injuries that would be subsequently seen and only now (years later) are gradually being acknowledged.
In turn, we are now seeing clear signs excess mortality has spiked across the globe, large polls are finding that one fifth of Americansknow someone they believe were killed by the vaccines and because so much trust has been lost from this cover up, public health authorities are at last admitting there may be a problem—but they didn’t say anything until now because they “didn’t want to create vaccine hesitancy,” which coincidently is the same excuse which has been used for decades (e.g., Dr. Meier, a distinguished professor called out this behavior after the government unleashed an easily preventable polio disaster in 1955.
Patterns of Vaccine Injury
I’ve had a long term interest in studying pharmaceutical injuries because many of my friends and relatives have had bad reactions to pharmaceuticals. In most of these cases, ample data existed to show that reaction could happen (often to the degree it strongly argued against the pharmaceutical remaining on the market) and yet almost no one in the medical field was aware of those dangers, hence leading to my injured friends never being warned before they took the pharmaceutical or even while the injury was occurring (e.g., the doctor said the reactions they’d never seen anyone have those reactions, that whatever was happening was due to anxiety, and that they would soon end—when in reality it became a lifelong condition because the patient didn’t stop the drug in time).
My bell curve theory originally came about from examining all of their cases. I thus was interested to know if the distribution of adverse events from the spike protein vaccines would match what I had observed with previous dangerous pharmaceuticals and if what I saw personally did or did not match what everyone was reporting online (which is part of why I put so much work into making sure the log was both accurate and detailed).
One of the things that immediately jumped out at me during that logging process were the multiple cases of a friend’s parent in a nursing home receiving the vaccine, immediately undergoing a rapid cognitive decline which was “diagnosed” as Alzheimer’s disease and then dying not long after. At the time, I assumed these were most likely due to undiagnosed ischemic strokes as that was the most plausible mechanism to describe what I’d heard, but I was not certain as I could never examine any of these individuals for signs a stroke had indeed happened.
Note: despite many deaths in the nursing home population due to COVID and the vaccines, the number of people awaiting admission to a nursing home has significantly increased (shown by this large data set from the Netherlands). Given that individuals typically do not want to go to a nursing home unless they are no longe able to take care of themselves, this suggests that something new is causing the rapid development of debilitating cognitive impairment (e.g., dementia) in the adult population. Likewise, as Ed Dowd has repeatedly documented, there has been a large increase in physical and cognitive disability throughout the adult population which has significantly impacted the economy because of how many workers are being lost to vaccine injuries.
Most recently, Steve Kirsch was contacted by a whistleblower who reported there has been a 25 fold increase in sudden dementia at the nursing home where she works. Similarly, like the cases shared with me, Kirsch has noted that (like me) he has frequently been contacted by relatives who reported a sudden onset of dementia in their beloved relative which was then swept under the rug. Furthermore, he has also collected numerous other forms of evidence corroborating this is indeed happening. These cases are really sad because the elders in nursing homes have very little ability to advocate for themselves, and most people will just write the cases off as “Alzheimers,” rather than seeing the red flag staring them in the face.
These cases were very concerning to me, as they signified (per the bell curve) that there was going to be a much larger portion of people who would develop less severe cognitive decline following vaccination.
Note: one of the most common types of injuries from pharmaceuticals are neurological injuries which both impair cognitive function and create psychiatric symptoms. This places patients in a difficult situation of being gaslighted by the medical system. This is because their doctors assume the psychiatric symptoms the patients are experiencing are the cause of their illness rather than a symptom of it, leading to the patient being told the illness is all in their head and continually referred for psychiatric help. One of the best examples with this occurred as a result of the abnormal heart rhythms (e.g., rapid anxiety provoking palpitations) caused by the vaccine damaging the heart which were consistently diagnosed as being a result of anxiety, even when a subsequent workup I requested showed heart damage was present. Remarkably, in the early era of vaccines, many doctors (as detailed here) acknowledged that vaccines caused neurological injuries which manifested as psychiatric symptoms, but now that recognition has been almost completely forgotten.
As I began seeing more and more signs of cognitive impairment following vaccination, I realized that what I observed mirrored what I previously seen with chronic inflammatory conditions such as mold toxicity, HPV vaccine injuries, and lyme disease. Some of the examples included:
•Many people reported having a “COVID” brain where it was just harder for them to think and remember things. I sometimes saw this occur after more severe cases of COVID, but more frequently after vaccination, along with many instance of patients who per their timeline clearly developed it from the vaccine but nonetheless believed it had come from COVID.
•These issues tended to be more likely to affect older adults, but younger ones were more likely to notice (and complain) about them. In the case of older adults, I typically learned about them from someone else who had observed the cognitive decline rather than directly from the individual.
•I saw numerous cases of vaccine injured individuals who had trouble remembering or recalling the word they knew expressed what they were trying to communicate (this is also a common mold toxicity symptom).
•I had friends and patients who told me their brain just didn’t work the same since they’d received the vaccine. As an example, a few colleagues told me they started losing the ability to remember basic things they needed to practice medicine (e.g., medication dosages for prescriptions). They shared that they were very worried they would need to take an early retirement and that they thought it came from the vaccine but there was no one they could talk to about it (which understandably created a lot of doubt and anxiety).
•I saw cases of coworkers demonstrating noticeable (and permanent) cognitive impairment after I’d assumed they’d received the vaccine. Their impairment was never mentioned or addressed (rather the physician kept on working, did not perform as well, and in some cases retired).
•I met significantly injured vaccine injured patients who told me one of the primary symptoms was a loss of cognitive functioning they had taken for granted throughout their life. In many cases following treatment of their vaccine injury, their cognition also improved.
•Colleagues who treated vaccine injured patients told me cognitive impairment was one of the common symptoms they saw and was particularly noteworthy because they had never seen anything like that happen to young adults. To quote Pierre Kory:
In my practice of treating vaccine injuries, one of the three most common symptoms I see is brain fog. So many of my patients had been in the prime of their lives, can now barely function, have significant cognitive impairment and need a lot of help from our nurses to carry out their treatment plans. I never imagined I would see any of this in people far younger than me and instead I see it every day. I bear witness to an immense amount of suffering on a daily basis that is hard to put into words.
•One of my friends (a very smart immunologist) developed complications from the first two vaccines and based on their symptoms was able to describe exactly which parts of their immune systems were becoming dysregulated. Against my advice, they took a booster and reported they suffered a significant cognitive impairment never experienced before in their lifetime. I feel this case was important to share as it illustrates how an exacerbation of a vaccine injury can also cause an exacerbation of cognitive symptoms.
Note: I also saw significant cognitive impairment occur in individuals who were acutely ill with COVID-19. This was not as unusual since delirium is a well known complication in patients hospitalized with a systemic illness (e.g., sepsis), but it seemed to happen more frequently than usual. However, in almost all cases, COVID-19 cognitive impairment resolved after their illness (even when they had been critically ill and required hospitalization) whereas the cognitive impairment I saw from the vaccines was often permanent (unless it was treated).
I specifically wanted to write this article for two reasons.
First, unless you’ve talked to a lot of people who have been through this, it’s really hard to describe what it’s like to gradually lose your mind and the basic cognitive function you relied upon to navigate the world—especially if everyone around you is telling you that it’s not happening and it’s all in your head. I wrote this article to give a voice to those people.
Second, despite Alzheimer’s disease being the mostly costly disease for America, most providers know fairly little about it and instead use it as a blanket diagnosis for anytime a patient shows signs of impaired cognition. This, I in turn would argue has been because there is minimal interest in understanding the causes (and treatments) of Alzheimer’s disease as there is so much more money in “research” for it and productive expensive (but useless and harmful) drugs for it.
Evidence of Cognitive Impairment
At the same time I was observing these effects, many rumors were also swirling around online that the vaccines would cause severe cognitive impairment and that we would witness a zombie apocalypse from the vaccine injuries.
This apocalypse of course never happened (which again illustrates why it is so important to be judicious with what one pronounces will come to pass—as our movement has repeatedly damaged its credibility by making easily outlandish and easily falsifiable predictions). Nonetheless, many have observed a suspicion cognitive impairment was occurring. For example to quote Igor Chudov’s article on the topic:
I own a small business and deal with many people and other small businesses. Most provided reliable service, would remember appointments, followed up on issues, and so on. I noticed that lately, some people have become less capable cognitively. They forget essential appointments, cannot concentrate, make crazy-stupid mistakes, and so on.
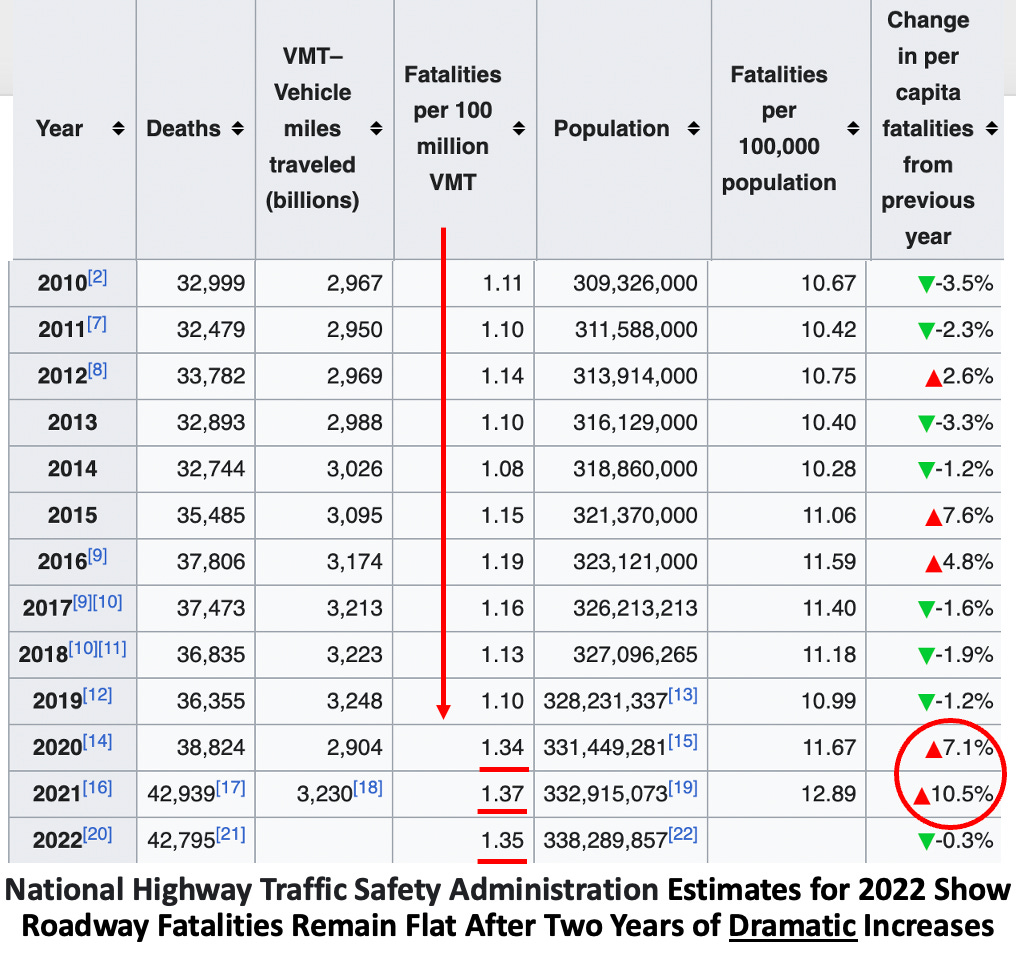
In my own case, in addition to poorly performing colleagues, the most evident change I noticed was a worsening of drivers around me and had quite a few near misses from impaired driving.
The great challenge with these situations is that it’s very hard to tell if something is actually happening or your perception is simply a product of confirmation bias. For this reason, while I was comfortable asserting my belief the COVID-19 vaccines were causing the severe injuries on either end of the bell curve, I avoided doing so for many of the less impactful injuries in the middle where it was much more ambiguous if what I was observing was “real” or simply my own biased perception of the events around me. Because of this, amongst other things, I never mentioned the changes in driving I observed.
Note: after I posted the original article many of the readers stated they too had observed a significant worsening in the behavior of drivers around them. I was then pointed to this dataset, which suggeststhis issue was happening, but is difficult to properly assess because COVID-19 can also cause cognitive impairment and less people were driving in 2020 and because the datasetstill has not been updated since 2022.
Recently, Igor Chudov was able to identify another dataset from the Netherlands which further corroborated that we were indeed facing a massive cognitive decline:
Primary care data for January to March 2023 showed that adults visited their GP more frequently for a number of symptoms compared to the same period in 2019. Memory and concentration problems were significantly more common than last year and in the period before COVID-19. Where these symptoms are concerned, the difference compared to 2019 is growing steadily in each quarter.
In the first quarter of 2023, there was a 24% increase in GP [general practioner] visits related to memory and concentration problems among adults (age 25 years and older) compared to the same period in 2020. This is evidenced by the latest quarterly research update from the GOR Network. The increase in memory and concentration problems of adults seems to be a longer-term effect of the coronavirus measures as well as SARS-CoV-2 infections.
More specifically they found:
•No increase was observed in adults under 25 years old.
•A 31% increase was observed in those 24-44 years old.
•A 40% increase was observed in those 45-74 years old.
•A 18% increase was observed in those over 75 years old.
Note: previous rounds of this survey, in addition to the cognitive issues described above, found that since 2019, the general population has also experienced worsening mental health (e.g, anxiety, depression or suicidal thoughts), sleep problems, tiredness, and cardiovascular issues (e.g., shortness of breath, dizziness or heart palpitation).
Typically, patients, less than 75 years old are unlikely to visit their doctors for cognitive issues. Taken in context with this data, it means there is a stronger case that the (massive) increases in cognitive issue for those under 75 were caused by something that happened after 2019. Additionally, since there were already a large number of visits for cognitive impairment in the elderly, the lower percentage increase is slightly misleading in quantifying the extent to which everyone was affected. For example to quote the previous report:
Primary care data showed that adults visited their GP somewhat more frequently for sleep problems in October–December 2022 than in the same period in 2019. This was particularly striking in the oldest age group (75 years and older).
Note: poor sleep is one of the primary causes of cognitive impairment (or dementia) and sadly also commonly impaired after COVID-19 vaccination.
All of this data put health officials in a bit of an awkward situation since publishing data demonstrating large scale cognitive impairment directly undermines the narrative they previous had committed themselves to. Nonetheless, the authors of the report were significantly more candid than many other before them:
The source of this increase in memory and concentration problems is unclear. A possible explanation could be that COVID-19 measures caused accelerated cognitive decline among people who were starting to have problems with memory and concentration (66 years on average).
COVID-19 was of course cited as a potential cause (which, as discussed above can sometimes cause long term cognitive impairment):
A supplementary explanation could be that some of these people have long-term symptoms after COVID-19. Various studies have shown that memory and concentration problems are common in post-COVID symptoms. Other infectious diseases, such as flu, can also cause these symptoms. However, recent studies have shown that long-term memory and concentration problems are much more common after COVID-19 than after flu. In addition, these symptoms are more common in older age groups. The figures provided by GPs are consistent with this expectation.
Fortunately, the authors acknowledged that long COVID could not be the primary explanation for what was occurring, and instead alluded to the elephant in the room—the vaccines.
Finally, Ed Dowd has identified numerous government datasets demonstrating that widespread impairment and disability has occurred since the vaccine rollout. Likewise, VAERS detected a massive spike in cognitive issues being reported to it after the COVID vaccines hit the market.
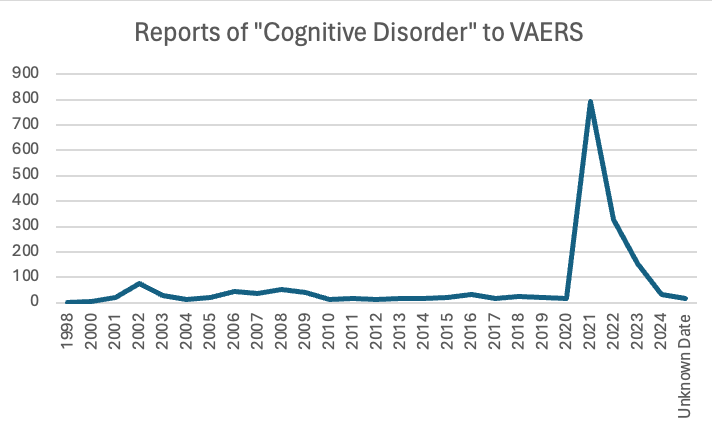
Note: one of the key components of the COVID-19 vaccine push was to make it politically incorrect to raise any data-based objections to the vaccines, and thereby stifle any inconvenient discussions of the topic which would have exposed how dangerous these products were. Because of this, I repeatedly heard stories (like this one) of liberals (including famous ones) who had severe vaccine injuries but could not discuss them with their peers, as doing so meant being outcasted from their social group and being cut off from job opportunities. Fortunately, things are now changing (as there are too many injuries to hide) and we are beginning to see more and more prominent individuals “come out of the closet” and admit they were vaccine injured.
Data Transparency
Making decisions has always been difficult and history is rife with catastrophic errors made by individuals who got it wrong. Because of this, a variety of solutions have been developed over the years (e.g., having a committee go through a process to decide something as it is unusual to have a leader who excels at making excellent decisions), all of which have serious short comings.
In recent years, we’ve had a push for data to become the means to making decisions. On one level, I think this is an excellent approach. For example in sales and the internet (which is where I suspect is where much of the push for data originated from), large amounts of data are used on a daily basis and constantly used to refine how a marketing campaign internet platform is set up so that it can maximize profits.
However, in many cases (e.g., those outside of business and sales), that same incentive to optimally utilize the data and adjust what’s being done due to the data does not exist. Because of this, while we have a large emphasis on gathering data, most of it is never utilized. For example, in medicine, we force our healthcare workers to do an immense amount of data entry, yet, we never comb the electronic health records to determine which drugs are unsafe or ineffective (which is very easy to do). I would argue this is because the healthcare systems receives so much unconditional money they have no incentive to produce better results and because the pharmaceutical industry receives so much money for toxic drugs, it has every incentive to keep them on the market.
In order to enshrine this paradigm, industry had to both create the mythology that data should both be viewed as the ultimate authority we must all be subservient to, but simultaneously not be something that is publicly available. This in turn was done by arguing that data was “costly proprietary information and intellectual property must be protected” or that it “contained personal health information which could not ethically be disclosed to protect the patients.”
In turn, science has very much become us being expect to trust the team of “experts” who analyze a dataset, and not surprisingly, this process lends itself to corruption.
For example, the only publicly available vaccine injury database VAERS exists because activists forced it to be required by law, and ever since it was made, the government (along with the medical establishment and the media) has done everything it can to undermine VAERS (discussed further here). Because VAERS reputation had been sullied, for the COVID vaccines, a new monitoring system, V-Safe, which was designed to address the short comings of VAERS was created. However, before long, activists discovered that V-safe did not allow the majority of adverse reactions to be reported in it, and furthermore would not make the data available for outside analysis. Instead, we were given access to a Lancet publication which concluded that:
Safety data from more than 298 million doses of mRNA COVID-19 vaccine administered in the first 6 months of the US vaccination programme show that most reported adverse events were mild and short in duration.
Reports of seeking medical care after mRNA vaccine were “rare”…Serious adverse events, including myocarditis, have been identified following mRNA vaccinations; however, these events are rare. Vaccines are the most effective tool to prevent serious COVID-19 disease outcomes and the benefits of immunisation in preventing serious morbidity and mortality strongly favour vaccination.
Through lawsuits, activists were eventually able to obtain the V-safe data where they then discovered the above study had lied and there were a lot of serious issues within that database. For example, the above article claimed 0.8-1.0% of vaccine recipients required medical care, whereas the raw V-safe data show 7.7% did—on average 2.7 times, which meant that every 4.8 vaccinations caused one medical visit.
Likewise, throughout the pandemic, we had almost all of the scientific journals refuse to publish anything which challenged the narrative (e.g., I’ve been in touch with numerous teams that have run into an endless number of roadblocks to publish contrarian data). Yet, simultaneously, those journals were willing to contort the existing (poor quality) data as much as possible if that supported the narrative (e.g., Pierre Kory has shown how multiple studies whose data demonstrated ivermectin benefitted patients concluded ivermectin was useless and then widely promoted for having debunked ivermectin).
Similarly, Deborah Birx and Anthony Fauci were essentially responsible for the disastrous COVID-19 response (e.g., useless but harmful mass testing, masking and lockdowns), as both within the White House and in the (fawning) media, they relentlessly and successfully pushed for those approaches regardless of how much protest they met. As both news clips and eye witnesses testimonies showed, Fauci and Birx constantly used “the data” to justify their their approach (e.g., when challenged, Birx would often say “I’m all about the data” while Fauci always cited “the data” whenever he advocated for a policy on national television).
However, Scott Atlas (who was with them on the White House COVID-19 task force) discovered that they both never presented scientific papers to the task force, lacked the ability to critically evaluate scientific research, they did not understand basic medical terminology, they would make patently absurd and non-sensical interpretations of their data, and adamantly refused to consider any of the data which challenged their narratives. In many cases, what he witnessed was so absurd he likened it to being in the Mad Hatter’s tea party from Alice and Wonderland, whereas I felt it was a real life version of this iconic Whitehouse scene from Idiocracy.
Because of the widespread lack of data transparency, a few different approaches exist.
First many (e.g., Drs. Peter Gøtzsche and Malcolm Kendrick) have gradually become experts in “data forensics” and being able to identify the tricks the pharmaceutical industry uses to doctor research so that the data always ends up supporting the sponsor’s desired conclusion. What I personally find depressing about this is that a fairly repetitive playbook is used to doctor studies, but the top medical journals consistently turn a blind eye to this, always publish that deceptive research, and in most cases refuse to correct it once the public points out the fraud.
Second, many (e.g., Steve Kirsch) argue that if data is not made publicly available, one must assume it’s incriminating and the data’s owners are lying about what’s in it (e.g., that the COVID vaccines are safe and effective). For example, for decades activists have been trying to get access to the data from the CDC’s Vaccine Safety Datalink (as it has the information which could definitively say if vaccines are safe or effective) but they’ve had no success—which in turn suggests that database is full of incriminating information for the vaccine program. Likewise, given the disconnect between what I was seeing with COVID-19 vaccine injuries and what the government was reporting (the only message we ever heard was “safe and effective!”) it was clear to me the government had very bad data and had made the decision to do whatever could be done to cover it up—a prediction which sadly has continued to hold true.
Third, we have to rely upon publicly available datasets which happened to capture the effects of vaccination programs (e.g., the one which tracks annual disability rates in the USA registered a huge spike after the COVID-19 vaccines hit the market). Unfortunately, while these clearly show that an issue exists which needs to be investigated, they do not definitively prove causality, and hence are often dismissed on that basis (much like VAERS is).
Fourth, we have to rely upon whistleblowers. Unfortunately, when this happens, the national government typically targets them for violating “patient confidentiality.” For instance, when a New Zealand whistleblower released fully anonymized data showing the vaccines were killing people, his government charged him with crimes carrying a maximum seven year prison sentence.
Note: the most recent example of government persecution of whistleblowers happened in Texas, where in February 2022, Texas’s government declared providing gender transitions to minors constituted child abuse, and June 2023, outlawed it. In response to this, in March of 2022, one of the largest Children’s hospitals in Texas (and where Peter Hotez exerts a significant amount of influence) announced it would stop providing transgender hormonal therapies. This however was a lie, so in April 2023, a concerned surgeon who had previously worked at the hospital convinced the hospital to give him access to their medical records, and then leaked anonymized medical records demonstrating that the hospital was continuing these practices, as in his opinion, under Texas law, this was child abuse he was required to report. In response to this, the Biden administration (not Texas) charged him with four felonies which carry a maximum penalty of 10 years in prison, which is very different from how other HIPPA violations have been handled. Likewise, more recently, after another nurse at the hospital exposed that the hospital was committing Medicaid fraud by billing for transgender care but labeling it as something else (as Texas’s Medicaid program does not permit for those practices to be reimbursed), after which the FBI was sent to interrogate (and likely intimidate) the nurse.
All of this hence leaves us in a very disorienting position—how do we know who to trust? In turn, I would argue one of the largest reasons so many people trust the audacious lies the government tells us is because the alternative (not knowing who or what to trust) is arguably even worse.
In my own case, I’ve developed a very simple rule for navigating the scientific literature (and many other sources of information as well).
Step 1. Determine the biases and conflicts of interest of the publication source (e.g., most medical journals and their editors take a lot of money from the pharmaceutical industry and hence do not want to upset their sponsors—an issue we sadly also see in the mainstream media).
Step 2. Determine if the conclusion of a published study agrees with, challenges, or is relatively neutral to it’s publisher’s bias.
Step 3. Use this formula:
•Agrees with publisher—high likelihood the study is wrong and it’s probably not worth your time to look into it.
•Disagrees with publisher—high likelihood the study is correct and that a very high bar had to be passed for it to be published (along with significant pressure being exerted behind the scenes).
•Relatively neutral for the publisher—you can take the paper at face value when you analyze its methods and conclusions to see if they had a reasonable way to derive their conclusion. Additionally, while the most prestigious medical journals are corrupt, this category is the one area they shine in and often ensure high standards were met for publication.
South Korea’s Data
In November 2023 and March 2024, some very interesting data emerged from a team of South Korean researchers where they looked at the electronic health records for a quarter and then half of the population in Seoul (2.2 million for the first study and then 4.3 million for the second) and then compared the rates of a variety of new (non-serious) medical conditions in those vaccinated and unvaccinated over three months. From this, they found a variety of medical conditions had a significant increase in the vaccinated. Those increases were as follows (with a range existing depending on how long after vaccination they were compared and which COVID vaccines they received).
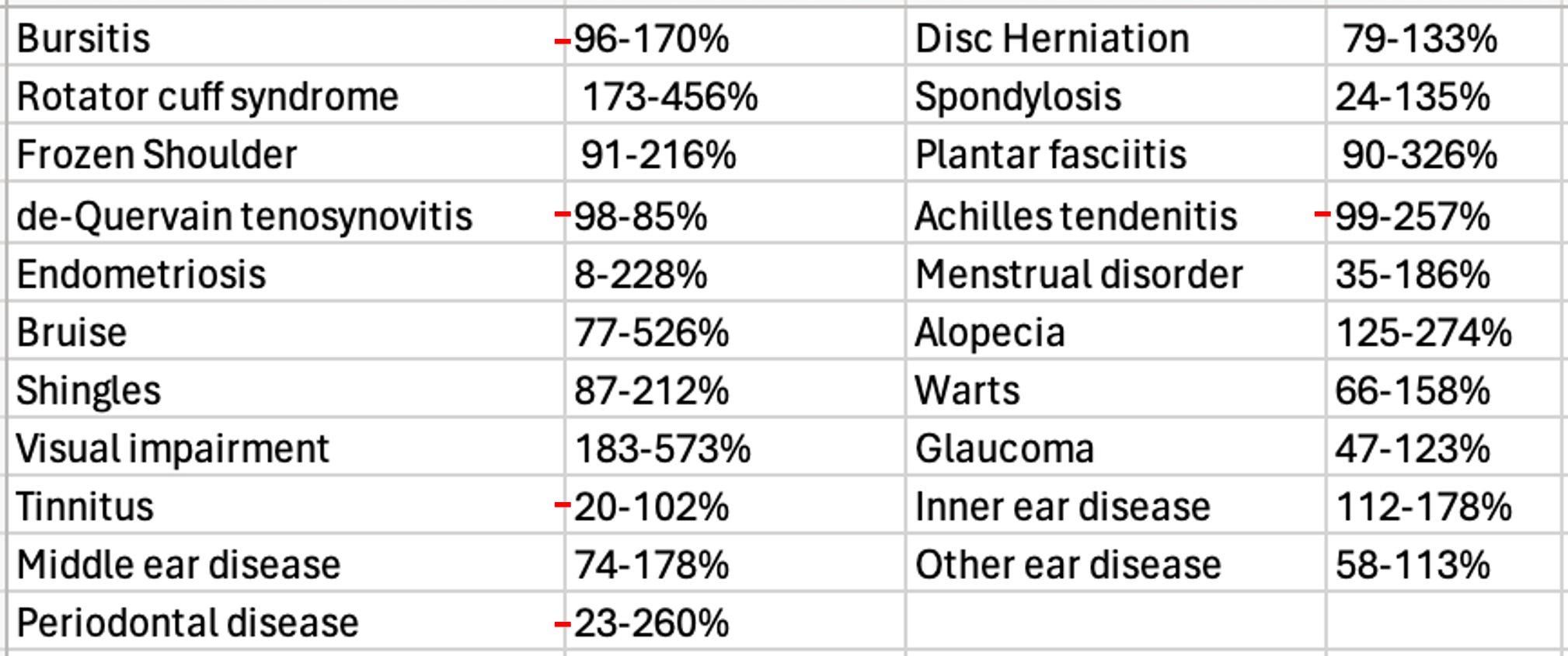
This was essentially a dataset we had been trying to get for over 2 years and it matched what we’d seen (e.g., many of these conditions such as shingles and alopecia [hair loss] appear to be strongly linked to vaccination). In turn, it both demonstrated that the vaccines were causing massive harm to society as millions of Americans suffer from these diseases and hence millions more developed them.
Unfortunately, after I analyzed them, I realized it was not appropriate for me to discuss them here as they were pre-prints rather than published articles, which either meant that they had fraudulent data (as it was quite extraordinary they got access to this data) or they were too politically incorrect for any journal to want to publish. While I felt the latter was much more likely, I was not sure which is was, so I avoided publishing that article (which was hard to do given how much time I’d put into it) as I did not want to fall into the trap of promoting something becauseit promoted my pre-existing biases and then misleading the audience here.
(BW: AMD included here the downloadable PDF files of the preprints but I don’t know how to attach them, so please go to his original article (link below) to get them.)
We hence tried to reach the authors (no success) and I patiently waited for the articles to leave the preprint server (which has still not happened).
However, recently. three other studies were published by same team using the same dataset. The first one, (also from March 2024) analyzed the increase of ten common autoimmune disorders (autoimmune hepatitis, ankylosing spondylitis, hashimoto thyroiditis, hypertension, inflammatory bowel disease, primary biliary cholangitis, rheumatoid arthritis, graves, vitiligo, lupus).
This one stated only vitiligo was increased (by 174%), so it seemed plausible to me it could have been published, as it made a token admission the vaccines were bad (as they had a rare side effect from a disease most people don’t know about). Then, when I looked at the data, I noticed a few of the other conditions appeared to have also been increased. In turn, since those increases weren’t mentioned in the article, I took that as a sign the article was deliberately omitting incriminating information from its conclusion so it could make it to publication (this happens a lot). Additionally, I was surprised the authors did not evaluate for polymyalgia rheumatica, as this seems to be one of the autoimmune disorders most distinctively associated with vaccination.
That article made me more confident the initial results were real—however since it was published in an obscure journal, I reserved judgement on it. Recently however, two very important ones came out.
Two weeks ago, the first was published in Nature (one of the top medical journals). It found that COVID vaccination resulted in a 68% increase in depression, a 44% increase in anxiety, dissociative, stress-related, and somatoform disorders, a 93.4% increase in sleep disorders, a 77% decrease in schizophrenia, and a 32.8% decrease in bipolar disorder. I was really surprised to see this be published, and took it as a sign there may have been a decision made to begin disclosing some of the harms of vaccination in the official medical literature. Additionally, I took this as an indication that this was an indirect admission neurologic issues also followed vaccination (due to the strong link between neurologic and psychiatric symptoms).
Note: the previously mentioned Israeli surveyfound that 4.5% of those who received a vaccine developed anxiety or depression, and 26.4% who already had either experienced an exacerbation of it.
Around the same time (three weeks ago) another article was published in a mainstream journal (or to be more exact “accepted for publication”). It analyzed individuals over 65 and found COVID vaccination increased the risk of mild cognitive impairment 138% and the risk of Alzheimer’s by 23%, and a smaller increase in vascular dementia and Parkinson’s disease the authors did not deem to be significant.
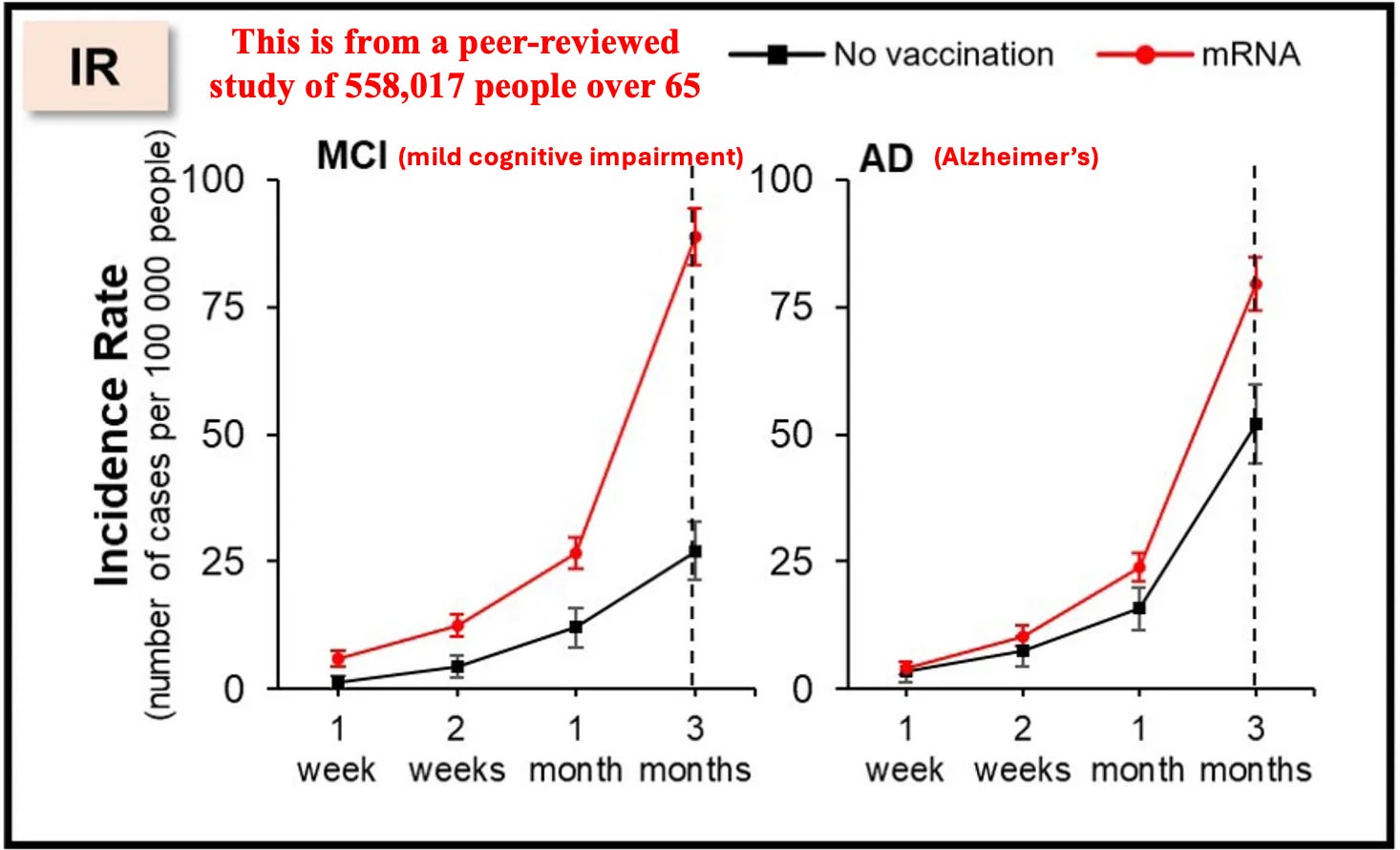
To put this in context, given that America spends over 300 billion dollars per year on Alzheimer’s disease, this single datapoint effectively means that the COVID vaccines cost the United States around 100 billion dollars. Additionally, as the authors only tracked the difference over 3 months (and it increased over time as these are both progressive diseases), the actual cost is likely greater, especially given that the elderly keep on receiving boosters. Likewise, it also makes a very strong argument for anyone who believes the vaccines damaged their cognition that this indeed happened.
Why Are The Vaccines Causing Cognitive Impairment?
My specific interest in studying spike protein vaccine toxicity arose because I suspected I would see many similarities to other pharmaceutical injuries I had observed previously and treatments that had developed for those injuries could be used to treat COVID-19 vaccine injuries. On Substack, I’ve tried to focus on explaining the areas that I believe are the most important to understanding this, zeta-potential, the cell danger response (CDR) and the treatments for Alzheimer’s disease. Note: Each of these is interrelated with and often causes the others.
Zeta Potential: Zeta potential (explained in detail here) governs if fluid in the body clumps together (e.g., forming a clot) or remains dispersed and capable of freely flowing. Additionally, it also influences if proteins will stay in their correct formation or misfold and clump together (with Alzheimer’s disease being characterized by misfolded proteins in the brain). Many different issues (discussed here) emerge when fluid circulation (be it blood, lymph, interstitial fluid or cerebrospinal fluid) becomes impaired. Since the spike protein is uniquely suited for impairing zeta potential, we have found restoring zeta potential(discussed here) often is immensely helpful during COVID-19 infections and for treating COVID-19 vaccine injuries. Many of those approaches in turn were initially developed from working with other vaccine injuries and cognitive decline in the elderly.
Note: the spike protein also has a prion forming domain, and many believe its responsible for the highly unusual amyloid (fibrous) blood clots seen in COVID-19 victims. Additionally, the COVID vaccines have been linked to extremely rare (and fatal) protein misfolding disorders such as the rapid dementia caused by CJD (discussed further here).
Cell Danger Response (CDR): When cells are exposed to a threat, their mitochondria shift from producing energy for the cell to a protective mode where the cell’s metabolism and internal growth shuts down, the mitochondria release reactive oxygen species to kill potential invaders, the cell warns other cells to enter the CDR and the cell seals off and disconnects itself from the body. The CDR (explained further here) is an essential process for cellular survival, but frequently in chronic illness, cells become stuck in it rather than allowing the healing response to complete.
Note: one common cause of impaired cognition are neurons becoming stuck in the CDR and hence not performing their cognitive tasks.
Understanding the CDR is extremely important when working with complex illnesses because it explains why triggers from long ago can cause an inexplicable illness, and why many treatments that seem appropriate (specifically those that treat a symptom of the CDR rather than the cause of it) either don’t help or worsen the patient’s condition. Many of the most challenging patients seen by integrative practitioners are those trapped within the CDR, but unfortunately, there is still very little knowledge of this phenomenon.
My interest was drawn back to the CDR after I realized that one of the most effective treatments for long COVID and COVID-19 vaccine injuries was one that systemically treated the CDR. Since many of the therapies that have been developed to revive nonfunctional tissue was developed by the regenerative medical field, I wrote an articledescribing how these approaches are applied to restore localized regions of dysfunctional tissue (which is sometimes needed to treat vaccine injuries) and another on the regenerative treatments that treat systemic CDRs (and are more frequently needed for vaccine injuries).
Alzheimer’s Disease (AD): since AD is one of the most costly disease in America, billions of dollars are spent each year in researching a cure for it. This research (which began in 1906) has had a very narrow focus on removing amyloid from the brain, and since the production of amyloid is a protective response from the brain, the decades of work to remove it have gone nowhere. Nonetheless, the FDA is presently working hand in hand with the drug industry to push forward ineffective, quite dangerous but highly profitable treatments for AD.
Remarkably, effective treatments do exist for AD and my colleagues have developed a few different methods that have successfully treated the condition. Additionally, one neurologist, Dale Bresden developed a method for reversing AD that he proved worked in mulitiple publications(included a recent 2022 clinical trial)—something which no one else has done, but remarkably has been almost completely ignored by the neurological field.
All of these successful approaches utilize the following principles:
•Restore both the blood flow to the brain and the lymphatic drainage from it (which safely removes amyloid plaques). This often requires restoring the physiologic zeta potential and having a healthy sleep cycle. Additionally, AD is commonly linked to damage to the lining of the brain’s blood vessels, which is unfortunate because one of the most frequent toxicities of the spike protein is injury to the blood vessels (which has been shown in many autopsies—including within the brain).
•Treating the CDR (which causes chronic inflammation) and reactivating brain cells that became trapped in an unresolved CDR (which amongst other things requires reclaiming a healthy sleep cycle, providing the nutrients the brain needs to sustain itself, and mitigating the damage of neurotoxins like inhaled anesthetics).
Note: Bresden’s approach also emphasizes the importance of addressing chronically elevated blood sugar or insulin levels.
One of the most important things to recognize about AD is that it is a slowly worsening disease which often progresses over decades. In the early stages of AD (where it is the most reversible), minor cognitive changes occur, which (when possible to autopsy) correlate with tissue changes within the brain. In rarer instances, individuals can instead have a rapidly progressing form of Alzheimer's (e.g., from Lyme) which strikes at a younger age and is often linked to the toxin exposure. Given how quickly the increase in AD appeared in both the patients I know and this dataset, I suspect it’s very likely the mechanisms behind the rapidly progressing forms of AD plays a key role in the cognitive impairment and dementia we are seeing from these vaccines.
Conclusion
Many of the most successful people I know are willing to go against a crowd and act in spite of being afraid (e.g., they resisted the peer pressure to get the vaccine because they felt it was a good idea). Likewise, rather than looking to an authoritative source for advice, they tend to create preliminary assessments of what’s going on based on the limited data that’s available to them, and then act on it rather than waiting for a clear and definitive answer (or at least a safe one) to present itself.
In turn, as I’ve gotten to know many of the prominent dissidents in this movement, I’ve found they all had those traits in common (which likewise many of my extraordinary medical mentors did as well). For example, Steve Kirsch used this capacity to become a successful Silicon Valley entrepreneur. When the vaccines came out, he “trusted the science,” and immediately got one, but before long noticed numerous people he knew had had severe injuries from them, and rather than be in denial about it, recognized that chain of injuries was statistically impossible, began digging into it, realized the existing data showed we had a huge problem, and then began speaking out on it despite the fact much of the (left wing) peer group he’d belonged to for decades disowned him for doing so.
In my own case, for the COVID vaccines, I had initially come in with expectation (which formed as the virus broke out in Wuhan) that whatever “emergency” vaccine was pushed for it would have significant issues and the adverse events would be by and large covered up by the government (or only “discovered” years down the line). In turn, I concluded it was far more preferable for me to feel confident I could treat the infection when I eventually got it and develop natural immunity than it was to take a risk with the vaccines.
However, once I began seeing a high number of red flags the moment the vaccines hit the market, I realized that I had made a big miscalculation and these things were incredibly dangerous so I needed to shift my focus to preventing people from being harmed by them.
Furthermore, I took the bell curve theory into account and assumed that if I was seeing occasional deaths or severe cognitive degeneration following vaccination, it was likely that far more cases of cognitive impairment were occurring, and as this recent Korean study shows, that is indeed the case.
It is thus both quite tragic and remarkable that we now have a leadership which has so little accountability to produce quality results that things like the basic scientific process (which helped our country become one of the most powerful nations in history) is being completely disregarded and replaced with a dogmatic system which refuses to consider basic data points which more and more are proving themselves to be immensely costly to our nation.
Everything we are seeing now was incredibly predictable and represented a systemic failure in our system and a profound societal declinethat must be reversed if we want our nation to be something which continues to provide the basic things we have taken for granted from it for most of our lives. I am especially worried as prior to COVID-19, our society was already struggling to reverse this decline, and since that time, we’ve been hit by a wave of cognitive impairment which can only further diminish our ability to address this.
Original article link:
Subscribe to A Midwestern Doctor’s unparalleled work:
A Midwestern Doctor says:
To learn how other readers have benefitted from this publication and the community it has created, their feedback can be viewed here. Additionally, an index of all the articles published in the Forgotten Side of Medicine can be viewed here.



No comments:
Post a Comment